

Last updated: July 2, 2026
Quick Answer: Emerging research has identified backwards-running nerve fibers, called “back channels,” that travel from the brain down to the cochlea and may amplify the phantom sounds associated with tinnitus. Innovative tinnitus treatments that block back channels in the ear aim to interrupt these signals using neuromodulation, targeted sound therapy, and other non-drug approaches. While most are still in clinical development, early results are promising for patients who haven’t found relief from traditional options. [3]
Key Takeaways
- 🔬 Back channels are efferent (brain-to-ear) nerve fibers that researchers now believe can feed abnormal signals back into the cochlea, worsening tinnitus.
- 🧠 Blocking or modulating these pathways is the core idea behind several innovative tinnitus treatments that block back channels in the ear.
- 🎛️ Bimodal neuromodulation (combining sound + mild electrical stimulation) is the most clinically advanced approach, with the Lenire device receiving regulatory clearance in some markets. [4]
- 💊 These treatments are non-drug and non-surgical, making them attractive to patients seeking alternatives.
- ⏱️ Most protocols require weeks to months of consistent use before measurable relief appears.
- 💰 Costs vary widely, from a few hundred to several thousand dollars, and insurance coverage is limited but growing.
- ✅ Good candidates tend to be adults with chronic, non-pulsatile tinnitus and no active middle ear disease.
- ⚠️ No treatment currently offers a guaranteed permanent cure; the goal for most patients is meaningful, lasting reduction in tinnitus loudness and distress.
What Are Back Channels in the Ear and How Do They Cause Tinnitus?
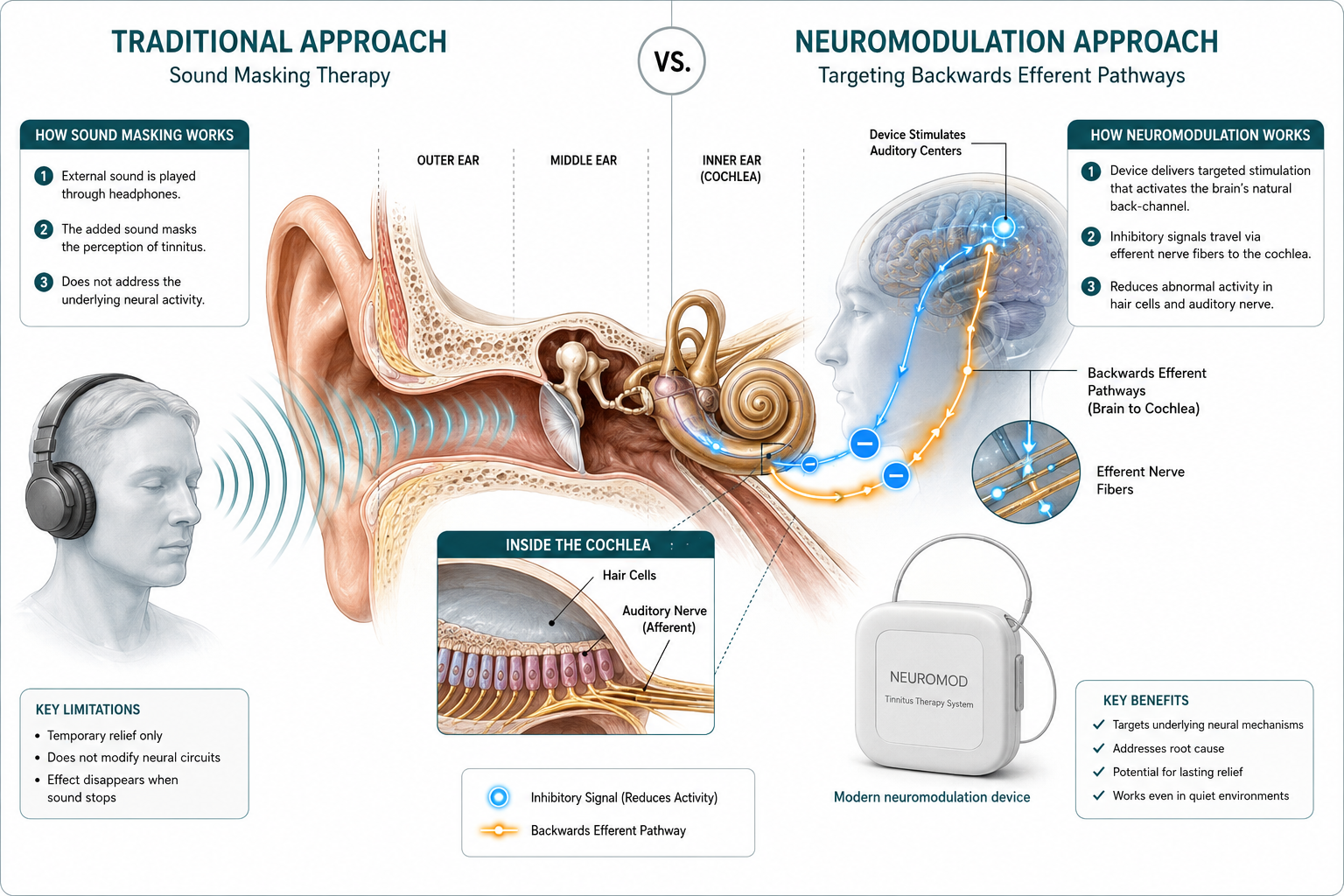
Back channels are efferent nerve fibers that run in the opposite direction of normal hearing signals — from the brain down to the cochlea (inner ear), rather than from the ear up to the brain. Recent basic research has identified these backwards nerve pathways as a potential contributor to both tinnitus and hyperacusis. [3]
In a healthy auditory system, efferent fibers help fine-tune how sensitive the cochlea is to sound. But when the auditory system is disrupted — by noise damage, aging, or other injury — these back channels may begin sending abnormal, amplified signals back to the ear. The result can be the phantom ringing, buzzing, or hissing that tinnitus sufferers experience, even in complete silence.
Why this matters:
- Traditional tinnitus models focused almost entirely on the ascending (ear-to-brain) pathway.
- Recognizing the descending (brain-to-ear) pathway opens a new target for treatment.
- Blocking or quieting these back-channel signals could reduce the “volume” of tinnitus at its source rather than just masking it. [3]
For a broader look at ear disorders and their neurological connections, the underlying anatomy helps explain why these pathways matter.
How Do Back Channel Blocking Treatments Work for Tinnitus?
Innovative tinnitus treatments that block back channels in the ear generally work by disrupting or re-training the efferent nerve signals that travel from the brain to the cochlea. The most studied mechanism uses bimodal neuromodulation, which pairs precisely timed auditory tones with mild electrical stimulation (usually to the tongue or skin) to recalibrate neural activity across both ascending and descending pathways. [7]
Key mechanisms being explored:
| Approach | How It Works | Development Stage |
|---|---|---|
| Bimodal neuromodulation | Sound + electrical pulse pairs retrain auditory circuits | Commercially available (some markets) |
| Transcranial magnetic stimulation (TMS) | Magnetic pulses target auditory cortex | Clinical trials |
| Vagus nerve stimulation (VNS) | Electrical stimulation paired with tones | Clinical trials |
| Targeted efferent suppression | Pharmacological or device-based inhibition of olivocochlear fibers | Early research |
The Lenire device, developed by Neuromod, pairs tonal sequences delivered through headphones with mild tongue-tip electrical stimulation. A clinical trial published in peer-reviewed literature found statistically significant reductions in tinnitus severity scores compared to control conditions. [4][5]
The vagus nerve also plays a role in auditory processing — see our guide on the vagus nerve and hearing for more context on how nerve stimulation affects sound perception.
Is Back Channel Blocking Better Than Traditional Tinnitus Treatment?
For many patients, yes — but with important caveats. Traditional treatments like sound masking, cognitive behavioral therapy (CBT), and hearing aids address tinnitus perception and distress without targeting the underlying neural mechanism. Back-channel-focused treatments aim to reduce the actual neural signal driving the phantom sound. [2][8]
Traditional vs. back-channel-blocking approaches:
- Sound masking/hearing aids: Effective for managing distress; do not change the underlying neural activity.
- CBT: Reduces tinnitus-related anxiety and improves quality of life; does not reduce tinnitus loudness.
- Back-channel blocking (bimodal neuromodulation): Targets the neural source; clinical data show reductions in both loudness and distress for a meaningful subset of patients. [5][9]
Choose back-channel approaches if: you have chronic tinnitus that hasn’t responded to masking or counseling, and you’re willing to commit to a structured multi-week protocol.
Stick with traditional approaches if: your tinnitus is mild, recently onset, or linked to a treatable cause like earwax or middle ear fluid (see otitis media with effusion).
What’s the Difference Between Back Channel Blocking and Sound Masking for Tinnitus?
Sound masking uses external noise (white noise, nature sounds, or broadband tones) to cover up tinnitus — the relief stops when the masking sound stops. Back-channel blocking treatments aim to create lasting changes in how the auditory nervous system behaves, so relief can persist after the device is removed. [9]
Think of it this way: masking is like turning up the radio to drown out a noise outside. Back-channel blocking is like fixing the source of the noise.
Are Back Channel Blocking Tinnitus Treatments FDA Approved?
As of 2026, no back-channel-specific tinnitus device has received full FDA approval in the United States, though several are in active review or trial phases. The Lenire bimodal neuromodulation device received CE marking in Europe and regulatory clearance in some other markets, and has been the subject of FDA Breakthrough Device designation discussions. [4][2]
Transcranial magnetic stimulation (TMS) devices have FDA clearance for depression but are used off-label for tinnitus in some clinics. Vagus nerve stimulation paired with sound therapy has shown strong clinical trial results and is moving toward regulatory submissions. [2]
Bottom line: Regulatory status is evolving quickly. Always confirm current approval status with a licensed audiologist or ENT specialist before starting any device-based protocol.
What Are the Side Effects of Back Channel Blocking Tinnitus Procedures?
Most non-invasive back-channel-blocking treatments have a favorable safety profile. The most commonly reported side effects from bimodal neuromodulation include mild tingling at the stimulation site (tongue or skin), temporary headache, and initial increases in tinnitus awareness during the adjustment period. [5][6]
Reported side effects by approach:
- Bimodal neuromodulation (Lenire): Mild tongue tingling, jaw discomfort, transient headache — generally self-resolving. [5]
- TMS: Scalp discomfort, headache, rare risk of seizure (very low with standard protocols).
- VNS: Neck discomfort, voice changes (with implanted devices); non-invasive versions have fewer risks.
Serious adverse events are rare across all non-invasive approaches. Patients with cochlear implants, pacemakers, or active middle ear disease should discuss contraindications with their provider.
Can Back Channel Blocking Cure Tinnitus Permanently?
No current treatment reliably cures tinnitus permanently for all patients. However, clinical data on bimodal neuromodulation show that a significant proportion of patients maintain reduced tinnitus severity for months after completing a treatment course. [5][9]
“The goal isn’t necessarily silence — it’s meaningful, durable reduction in how much tinnitus disrupts daily life.”
Research from the University of Minnesota’s Sonic Lab found that bimodal neuromodulation produced lasting improvements in tinnitus handicap inventory scores in a substantial portion of participants. [7] Long-term follow-up data (beyond 12 months) are still accumulating.
Who Is a Good Candidate for Back Channel Blocking Tinnitus Treatment?
Adults with chronic, non-pulsatile tinnitus lasting more than six months are the primary target population. Candidates typically have normal or near-normal middle ear function and have not found sufficient relief from hearing aids, masking, or counseling alone. [8]
Good candidates:
- Chronic tinnitus (6+ months)
- Tinnitus linked to noise exposure or age-related hearing changes
- No active middle ear infection or fluid (see symptoms of ear nerve damage)
- Motivated to complete a multi-week protocol
Less suitable candidates:
- Pulsatile tinnitus (may indicate a vascular cause requiring separate evaluation)
- Active Menière’s disease with fluctuating hearing (learn more about Menière’s disease)
- Cochlear implant users (device interference risk)
- Children and adolescents (insufficient safety data)
How Long Does It Take to See Results From Back Channel Blocking Treatment?
Most clinical protocols for bimodal neuromodulation run 12 weeks, with patients using the device for 30–60 minutes daily. Meaningful improvements in tinnitus severity scores typically emerge between weeks 6 and 10 of consistent use. [5][7]
Some patients notice modest changes within the first few weeks; others don’t see significant benefit until after completing the full course. Rushing or skipping sessions is one of the most common reasons for poor outcomes.
What Are Alternatives to Back Channel Blocking for Tinnitus Relief?
Several well-supported alternatives exist for patients who aren’t candidates for back-channel-blocking approaches or who want to combine strategies:
- Hearing aids with tinnitus masking features — especially effective when tinnitus accompanies hearing loss. See advanced hearing aids for tinnitus relief.
- Cognitive behavioral therapy (CBT) — the most evidence-backed psychological approach for tinnitus distress. [8]
- Tinnitus retraining therapy (TRT) — combines counseling with low-level broadband sound.
- Natural and lifestyle approaches — stress reduction, sleep hygiene, and dietary changes. See natural remedies for tinnitus.
- AI-assisted audiological tools — emerging platforms for personalized tinnitus profiling. See AI tools transforming hearing loss diagnosis.
How Much Does Back Channel Blocking Tinnitus Treatment Cost?
Costs vary considerably depending on the device and delivery model. The Lenire device, when available through licensed audiologists, has been priced in the range of $2,500–$4,000 USD for a full treatment course including professional fitting and follow-up. [4] TMS sessions in clinical settings typically run $150–$300 per session, with a standard course involving 10–20 sessions.
These are estimates based on publicly available pricing; actual costs depend on geography, provider, and insurance status.
Is Back Channel Blocking Tinnitus Treatment Covered by Insurance?
Most private insurers in the US currently classify bimodal neuromodulation devices as investigational or experimental, which limits reimbursement. Coverage is more common in some European markets where regulatory approval is established. [2]
Practical steps to pursue coverage:
- Request a letter of medical necessity from your ENT or audiologist.
- Check whether your plan covers “tinnitus rehabilitation devices” as a category.
- Ask about flexible spending account (FSA) or health savings account (HSA) eligibility — most qualifying medical devices are FSA/HSA eligible.
- Monitor insurer policy updates, as FDA clearance decisions often trigger coverage reviews.
What Happens if Back Channel Blocking Doesn’t Work for My Tinnitus?
Non-response is real — clinical trials show that a meaningful minority of patients do not experience significant improvement from bimodal neuromodulation. [5] If back-channel-blocking treatment doesn’t deliver results after a full protocol, the next steps include:
- Comprehensive audiological re-evaluation to rule out treatable causes (e.g., hearing loss in one ear)
- Trial of a different neuromodulation modality (e.g., TMS or VNS)
- Structured CBT program with a tinnitus-specialist psychologist
- Combination therapy pairing masking with counseling
Non-response to one approach doesn’t mean all options are exhausted.
Common Mistakes People Make With Back Channel Blocking Tinnitus Treatments
- Inconsistent use: Skipping daily sessions significantly reduces cumulative neural retraining effects.
- Unrealistic expectations: Expecting complete silence rather than meaningful reduction leads to premature abandonment.
- Skipping audiological assessment: Starting a device without ruling out treatable causes (earwax, fluid, vascular issues) wastes time and money.
- Self-diagnosing tinnitus type: Pulsatile tinnitus requires vascular workup before any neuromodulation trial.
- Combining unverified supplements without guidance: Some supplements interact with auditory function. Check hearing support supplements for evidence-based options.
FAQ
Q: What exactly are “back channels” in the ear? Back channels are efferent (outgoing) nerve fibers that run from the brain down to the cochlea. Unlike the main auditory nerve, which carries sound signals up to the brain, these fibers carry signals in the reverse direction and can influence cochlear sensitivity. [3]
Q: Is bimodal neuromodulation the same as back-channel blocking? Not exactly — bimodal neuromodulation targets overall auditory neural plasticity, including efferent pathways. Back-channel blocking is a more specific concept focused on suppressing abnormal efferent signals. Bimodal neuromodulation is currently the most practical clinical application of this research. [7]
Q: How is the Lenire device different from a standard hearing aid? Lenire is not a hearing aid. It delivers paired auditory tones and tongue-tip electrical pulses to retrain auditory circuits. Hearing aids amplify sound to compensate for hearing loss; Lenire aims to reduce tinnitus severity through neural recalibration. [4]
Q: Can tinnitus caused by noise damage respond to back-channel blocking? Yes. Noise-induced tinnitus is one of the most studied subtypes in bimodal neuromodulation trials, and this group tends to show favorable response rates. [5][9]
Q: Is there an age limit for these treatments? Most clinical trials have enrolled adults aged 18–75. There is insufficient safety and efficacy data for children and adolescents. Older adults with age-related hearing changes are generally eligible. [8]
Q: Do I need a prescription or referral? In most markets, access to regulated neuromodulation devices requires evaluation by a licensed audiologist or ENT physician. Self-purchasing unregulated devices online is not recommended.
Q: How does stress affect back-channel tinnitus signals? Stress activates the autonomic nervous system, which can increase efferent activity and amplify tinnitus perception. Stress management is often recommended alongside neuromodulation therapy. [10]
Q: Can I use noise-cancelling headphones while undergoing back-channel treatment? Generally yes, but check with your provider. Excessive noise suppression during treatment sessions may interfere with the auditory component of the protocol.
Q: Are there any home-based back-channel blocking options? Some commercially available sound therapy apps claim to target efferent pathways, but evidence for home-use apps is weaker than for clinically supervised device protocols. Supervised treatment remains the standard.
Q: What research institutions are leading this work? The University of Minnesota’s Sonic Lab is a prominent center for bimodal neuromodulation research. Karolinska Institutet has published foundational work on tinnitus neuroscience. [7][10]
Conclusion
Innovative tinnitus treatments that block back channels in the ear represent one of the most scientifically grounded new directions in tinnitus research. By targeting the efferent nerve fibers that carry signals from the brain back to the cochlea, these approaches go beyond symptom management and aim to address a root neural mechanism.
Actionable next steps:
- Get a full audiological evaluation before pursuing any device-based treatment — rule out treatable causes first.
- Ask your audiologist specifically about bimodal neuromodulation and whether you meet the criteria for a supervised trial.
- Check current regulatory status of devices in your country, as approvals are changing rapidly in 2026.
- Combine approaches — neuromodulation works best alongside CBT or tinnitus retraining therapy for most patients.
- Track your symptoms using a validated tool like the Tinnitus Handicap Inventory so you can measure real progress.
For a solid foundation, start with our complete guide to understanding tinnitus and explore tinnitus help and relief options to build a comprehensive management plan.
References
[1] PMC3136369 – https://pmc.ncbi.nlm.nih.gov/articles/PMC3136369/ [2] New Emerging Therapies – https://www.ata.org/about-tinnitus/therapy-and-treatment-options/new-emerging-therapies/ [3] Tinnitus Treatment Blocking Back Channels Ear – https://refractor.io/biology/tinnitus-treatment-blocking-back-channels-ear/ [4] Lenire – https://www.lenire.com [5] PMC10603282 – https://pmc.ncbi.nlm.nih.gov/articles/PMC10603282/ [6] PMC10607630 – https://pmc.ncbi.nlm.nih.gov/articles/PMC10607630/ [7] Sonic Lab Advancing Tinnitus Treatment Through Bimodal Neuromodulation – https://med.umn.edu/ent/news/sonic-lab-advancing-tinnitus-treatment-through-bimodal-neuromodulation [8] Mayo Clinic Tinnitus Diagnosis and Treatment – https://www.mayoclinic.org/diseases-conditions/tinnitus/diagnosis-treatment/drc-20350162 [9] New Tinnitus Therapy Can Quiet Torturous Ringing In The Ears – https://www.scientificamerican.com/article/new-tinnitus-therapy-can-quiet-torturous-ringing-in-the-ears/ [10] New Knowledge On Tinnitus Gives Hope – https://ki.se/en/research/popular-science-and-dialogue/spotlight-on/spotlight-on-our-senses/new-knowledge-on-tinnitus-gives-hope