
Last updated: June 26, 2026
Quick Answer: Research published between 2021 and 2026 reveals a genuine emerging link between metabolic liver disease and sudden hearing loss. People with metabolic dysfunction-associated steatotic liver disease (MASLD) or metabolic syndrome face a measurably higher risk of sudden sensorineural hearing loss (SSNHL), and those who do experience it tend to recover hearing less completely. The connection runs through systemic inflammation, vascular damage, and a weakened blood-labyrinth barrier in the inner ear.
Key Takeaways
- 🔬 Adults 65+ with MASLD have a 5% higher risk of developing sudden sensorineural hearing loss (SSNHL) compared to those without the disease [1]
- 🔥 Metabolic syndrome makes a person 1.88 times more likely to develop SSNHL, and recovery outcomes are significantly worse [4]
- 👂 Liver fibrosis markers (FIB-4 index, APRI) correlate with more severe hearing loss in SSNHL patients [3]
- 🩸 MASH (metabolic-dysfunction-associated steatohepatitis) can weaken the blood-labyrinth barrier in the cochlea, making the inner ear more vulnerable [2]
- 📉 SSNHL patients with metabolic syndrome had only a 22.9% hearing recovery rate vs. 42.6% in those without it [5]
- ⚠️ Sudden hearing loss is a medical emergency — treatment within 72 hours dramatically improves outcomes
- 🩺 Both an audiologist and a hepatologist may be needed; neither specialist alone covers the full picture
- ✅ Managing metabolic liver disease through diet, exercise, and medication may reduce hearing loss risk
What Is the Connection Between Liver Disease and Hearing Loss?
Metabolic liver disease and sudden hearing loss share a common thread: systemic inflammation and vascular dysfunction. When the liver is damaged by fat accumulation and metabolic stress, it releases inflammatory signals that circulate throughout the body, including to the delicate structures of the inner ear.
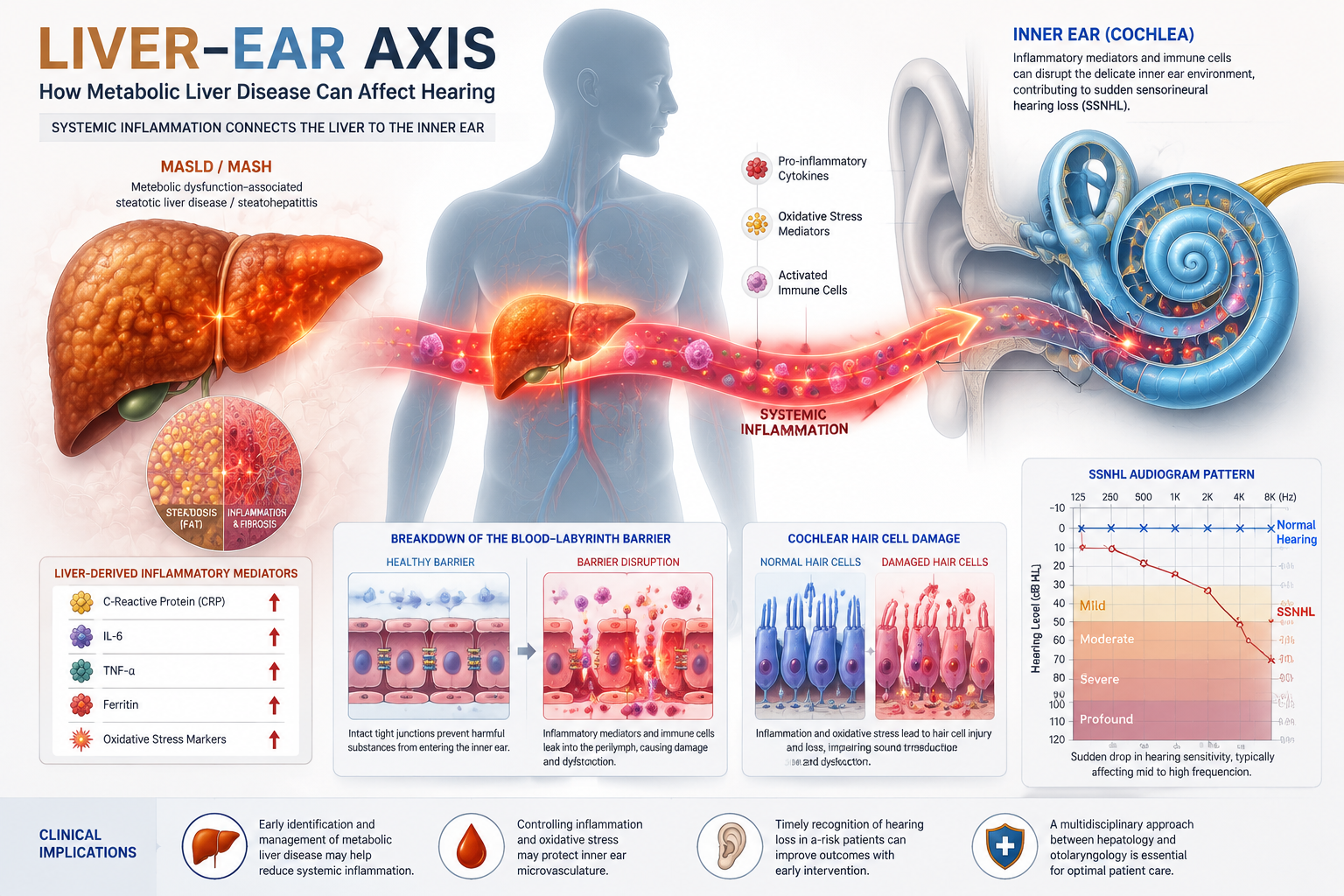
Researchers now refer to this pathway as the “liver-ear axis” — a concept supported by multiple studies showing that people with MASLD or MASH (its more advanced inflammatory form) have measurably compromised cochlear health [2]. The cochlea, the spiral-shaped hearing organ, relies on a tightly controlled blood supply and a protective barrier called the blood-labyrinth barrier. Metabolic liver disease appears to weaken both.
Key mechanisms include:
- Chronic low-grade inflammation damaging cochlear hair cells
- Reduced blood flow to the inner ear due to metabolic vascular changes
- Oxidative stress impairing auditory nerve function
- Elevated liver fibrosis markers correlating with worse hearing outcomes [3]
Can Fatty Liver Disease Cause Sudden Hearing Loss?
Yes — fatty liver disease, particularly in its advanced inflammatory form (MASH), is associated with a higher risk of SSNHL. A June 2025 study found that adults 65 and older with MASLD had a 5% greater risk of developing SSNHL compared to peers without the condition [1].
This doesn’t mean fatty liver directly causes hearing loss in every case. Rather, the metabolic dysfunction that drives liver disease also damages the inner ear over time. Think of it as two organs suffering from the same underlying problem: poor metabolic health.
“The same metabolic forces that scar liver tissue appear to quietly compromise the cochlea’s ability to withstand stress.” — supported by research published March 2026 [2]
Who should pay attention most:
- People with NAFLD/MASLD who are over 50
- Those with both liver disease and metabolic syndrome (high blood pressure, high blood sugar, high triglycerides)
- Anyone who notices sudden muffled hearing or sudden hearing loss in one ear alongside a known liver condition
How Does Metabolic Dysfunction Affect Hearing?
Metabolic dysfunction affects hearing through at least three overlapping pathways: inflammation, vascular damage, and oxidative stress.
1. Inflammation: MASH triggers the release of pro-inflammatory cytokines. These molecules travel through the bloodstream and can reach the cochlea, damaging hair cells that convert sound vibrations into nerve signals. Research from March 2026 confirmed that MASH impairs cochlear integrity and delays auditory recovery after noise trauma [2].
2. Vascular damage: The inner ear is fed by a single end artery with no backup circulation. Metabolic syndrome components — high blood pressure, insulin resistance, dyslipidemia — narrow and stiffen these vessels, reducing oxygen delivery to cochlear tissue.
3. Blood-labyrinth barrier breakdown: Similar to the blood-brain barrier, the blood-labyrinth barrier protects the cochlea from harmful substances. MASH weakens this barrier, leaving the inner ear exposed to inflammatory molecules and toxins [2].
For related reading on how systemic factors affect hearing, see this guide on hearing loss and cognitive decline — many of the same vascular risks apply.
What Are the Symptoms of Metabolic Liver Disease?
Metabolic liver disease is often called a “silent” condition because most people have no symptoms in the early stages. This is part of what makes the emerging link between metabolic liver disease and sudden hearing loss so concerning — both conditions can progress without obvious warning signs.
Common symptoms when they do appear:
| Stage | Symptoms |
|---|---|
| Early MASLD (fatty liver) | Usually none; mild fatigue possible |
| MASH (inflammation) | Fatigue, right upper abdominal discomfort, mild jaundice |
| Advanced fibrosis/cirrhosis | Swelling in legs/abdomen, easy bruising, confusion, jaundice |
Metabolic syndrome symptoms (often co-occurring):
- Abdominal obesity (waist over 35 inches in women, 40 in men)
- High blood pressure (130/85 mmHg or above)
- Elevated fasting blood sugar
- High triglycerides, low HDL cholesterol
Because symptoms are subtle, routine blood tests — including liver enzyme panels — are often how MASLD is first detected.
What Are the Causes of Sudden Sensorineural Hearing Loss?
SSNHL is defined as a rapid loss of 30 decibels or more across three consecutive frequencies, occurring within 72 hours. It affects roughly 5 to 27 per 100,000 people per year (estimates vary by study population), and in most cases, no single cause is identified.
Known and suspected causes include:
- Vascular: Reduced blood flow to the cochlea (most common suspected cause)
- Viral infections: Herpes simplex, mumps, cytomegalovirus
- Autoimmune conditions: The immune system attacks inner ear tissue
- Metabolic factors: Metabolic syndrome, diabetes, liver disease [4]
- Acoustic trauma: Sudden loud noise exposure
- Structural: Acoustic neuroma, perilymph fistula
Metabolic causes are gaining attention because they’re modifiable — unlike genetics or viral exposure, metabolic health can be actively managed. For a broader look at sudden deafness in one ear, including emergency treatment steps, that resource covers the full clinical picture.
Is Hearing Loss Reversible If Caused by Liver Disease?
Partial recovery is possible, but metabolic liver disease significantly reduces the odds. A 2018 study found that SSNHL patients with metabolic syndrome recovered hearing only 22.9% of the time, compared to 42.6% in those without metabolic syndrome [5].
Factors that improve recovery chances:
- Starting corticosteroid treatment within 72 hours of onset
- Younger age at time of hearing loss
- Less severe initial hearing loss
- Better-controlled metabolic health at the time of the event
Factors that worsen prognosis:
- Higher liver fibrosis scores (FIB-4, APRI) [3]
- Uncontrolled diabetes or hypertension
- Delayed treatment (beyond 2 weeks significantly reduces recovery)
The bottom line: if you have metabolic liver disease and notice sudden hearing changes, treat it as an emergency. Don’t wait to see if it resolves on its own. Also be aware that conditions like Ménière’s disease can mimic SSNHL and may also be influenced by metabolic factors.
How Common Is Hearing Loss With Liver Problems?
The exact prevalence is still being established, but the data so far points to a meaningful association. A 2021 meta-analysis found that people with metabolic syndrome — which frequently accompanies liver disease — were 1.88 times more likely to develop SSNHL [4]. A 2015 case-control study in Taiwan also identified metabolic syndrome as a significant risk factor for SSNHL [6].
Among older adults specifically, the risk appears higher. The 2025 study focusing on adults 65+ with MASLD found a statistically significant 5% elevated SSNHL risk [1]. While 5% may sound modest, at a population level — given how common MASLD has become — this translates to a large number of affected individuals.
What Tests Diagnose Liver-Related Hearing Loss?
No single test confirms that hearing loss is caused by liver disease. Instead, clinicians piece together findings from both liver and auditory evaluations.
Liver-side tests:
- Liver function tests (LFTs): ALT, AST, GGT
- FIB-4 index: Calculated from age, AST, ALT, and platelet count — higher scores indicate more fibrosis [3]
- APRI score: AST-to-platelet ratio; elevated scores correlate with worse SSNHL outcomes [3]
- Liver ultrasound or MRI: Assesses fat content and structural changes
- Liver biopsy: Gold standard for staging fibrosis
Hearing-side tests:
- Pure tone audiometry: Quantifies the degree and frequency pattern of hearing loss
- Speech discrimination testing: Assesses how well words are understood
- MRI of the internal auditory canal: Rules out acoustic neuroma or structural causes
- ABR (auditory brainstem response): Tests nerve pathway integrity
Connecting both sets of results helps identify whether metabolic factors are likely contributors. Recognizing hearing loss symptoms early is the first step before any formal testing.
Can You Prevent Hearing Loss From Liver Disease?
Prevention is genuinely possible because the underlying metabolic risk factors are modifiable. Managing MASLD aggressively reduces systemic inflammation, which in turn may protect the cochlea.
Evidence-based steps to reduce risk:
- Lose 5–10% of body weight if overweight — this alone can significantly reduce liver fat and inflammation
- Control blood sugar through diet, exercise, and medication if needed
- Manage blood pressure and cholesterol with lifestyle changes and, where appropriate, statins or other agents
- Limit alcohol — even moderate drinking accelerates liver fibrosis
- Exercise regularly — 150 minutes of moderate aerobic activity per week improves both liver and vascular health
- Get annual hearing checks if you have MASLD, metabolic syndrome, or diabetes
- Protect your ears from loud noise — a damaged cochlea is less resilient when also under metabolic stress
Hearing support supplements are sometimes discussed in this context, but evidence for their direct impact on metabolic hearing loss remains limited. See this overview of hearing support supplements for a balanced look.
Who Is at Risk for Metabolic Liver Disease and Hearing Loss?
The overlap between risk groups for MASLD and SSNHL is striking. People who fit multiple categories below face compounded risk.
High-risk profile:
- Adults over 50, especially 65+ [1]
- People with obesity, particularly central/abdominal obesity
- Type 2 diabetes or insulin resistance
- Metabolic syndrome (three or more of: high waist circumference, high triglycerides, low HDL, high blood pressure, elevated fasting glucose)
- Sedentary lifestyle
- Family history of liver disease or cardiovascular disease
Additional hearing-specific risk factors:
- History of noise exposure
- Prior episodes of tinnitus or ear fullness (see understanding tinnitus for context)
- Existing age-related hearing changes
What’s the Difference Between Metabolic and Viral Causes of Hearing Loss?
Both metabolic and viral causes can trigger SSNHL, but they differ in onset pattern, treatment, and prognosis.
| Feature | Metabolic Cause | Viral Cause |
|---|---|---|
| Onset | Often gradual vascular damage, acute event | Sudden, often with flu-like prodrome |
| Age group | More common in middle-aged/older adults | Any age |
| Associated symptoms | Tinnitus, metabolic syndrome signs | Fever, fatigue, recent illness |
| Recovery rate | Lower (especially with metabolic syndrome) [5] | Variable; often better in younger patients |
| Treatment focus | Steroids + metabolic management | Steroids + antivirals in some cases |
| Prevention | Yes — metabolic control | Partial — vaccination where applicable |
The distinction matters clinically because metabolic causes point toward long-term lifestyle and medical management, while viral causes may resolve more fully with acute treatment alone.
How Quickly Does Metabolic Liver Disease Progress?
MASLD can remain stable for years, but progression to MASH and then to fibrosis or cirrhosis is possible — and the timeline varies widely based on individual risk factors.
General progression timeline (estimates):
- Simple fatty liver (MASLD): May stay stable for 10–20 years in some people
- MASH (inflammation): Can develop within years of fatty liver onset, especially with metabolic syndrome
- Significant fibrosis: May develop over 5–10 years of uncontrolled MASH
- Cirrhosis: Advanced stage; typically takes decades but can accelerate with heavy alcohol use, diabetes, or obesity
The cochlear damage associated with liver disease likely accumulates alongside fibrosis. This is why higher FIB-4 and APRI scores correlate with worse hearing loss severity — more liver damage means more systemic inflammation over a longer period [3].
Should You See an Audiologist or Hepatologist First?
See an audiologist (or go to an emergency room) first if hearing loss is sudden — SSNHL is a time-sensitive emergency. Then follow up with a hepatologist or your primary care physician to evaluate liver and metabolic health.
Decision guide:
- Sudden hearing loss in the last 72 hours? → Emergency room or ENT immediately
- Gradual hearing changes + known liver disease? → Audiologist for baseline testing, then hepatologist for liver staging
- Metabolic syndrome without hearing symptoms? → Primary care physician for liver screening + annual hearing check
- Both liver disease and hearing loss confirmed? → Co-management between audiologist and hepatologist, with primary care coordinating
The emerging link between metabolic liver disease and sudden hearing loss means these two specialties need to communicate. Ask your doctors directly whether your liver health could be contributing to your hearing changes — it’s a question many clinicians haven’t yet connected.
Metabolic Liver Disease Treatment Options
Treatment for MASLD and MASH focuses on reducing liver fat, inflammation, and fibrosis. As of 2026, options include lifestyle interventions and a growing number of approved medications.
Lifestyle (first-line for all stages):
- Weight loss (5–10% body weight reduces liver fat; 10%+ can reverse MASH)
- Mediterranean-style diet
- Regular aerobic and resistance exercise
- Alcohol elimination
Medications:
- GLP-1 receptor agonists (e.g., semaglutide): Approved for weight loss and showing strong results in MASH trials
- Resmetirom (Rezdiffra): FDA-approved in 2024 specifically for MASH with fibrosis — the first drug approved for this indication
- Statins: Reduce cardiovascular risk and may have anti-inflammatory liver benefits
- Vitamin E: Used in non-diabetic MASH patients in some guidelines
For hearing loss specifically:
- Corticosteroids (oral or intratympanic injection) remain the standard treatment for SSNHL
- Managing metabolic risk factors improves prognosis for recovery
Frequently Asked Questions
Q: Can NAFLD cause tinnitus as well as hearing loss? A: Tinnitus (ringing in the ears) can accompany SSNHL, and metabolic dysfunction is a plausible contributing factor. However, direct evidence linking NAFLD specifically to tinnitus is limited. People with metabolic syndrome who experience tinnitus should have both liver and hearing health evaluated.
Q: Does alcohol-related liver disease carry the same hearing risk as metabolic liver disease? A: Alcohol-related liver disease involves different mechanisms but also causes systemic inflammation and vascular damage. Both types of liver disease can impair cochlear health, though the research on the metabolic-hearing link is more developed.
Q: How soon after SSNHL onset should I seek treatment? A: Within 24–72 hours. Treatment with corticosteroids is most effective in this window. After two weeks, recovery rates drop significantly.
Q: Is the liver-ear axis a proven concept or still theoretical? A: It’s supported by multiple studies as of 2026 but is still considered an emerging area of research. The mechanisms are plausible and the associations are statistically significant, but large-scale clinical trials are ongoing [2].
Q: Can children with liver disease develop hearing loss from it? A: Pediatric MASLD is rising, but the hearing loss connection has been studied primarily in adults. Children with metabolic liver disease should have regular hearing screenings as a precaution.
Q: Does losing weight improve hearing if metabolic liver disease is the cause? A: Directly reversing hearing loss through weight loss is not established. However, reducing liver inflammation may slow further cochlear damage and improve the odds of recovery from future SSNHL events.
Q: Are there specific blood tests that predict hearing loss risk in liver disease patients? A: Yes — elevated FIB-4 index and APRI score are associated with more severe hearing loss in SSNHL patients [3]. These are standard liver fibrosis markers available through routine blood work.
Q: Can vertigo accompany metabolic hearing loss? A: Yes. Inner ear damage from any cause can affect both hearing and balance. For more on this connection, see vertigo and hearing loss.
Q: Is sudden hearing loss from metabolic causes more likely in one ear or both? A: SSNHL typically affects one ear. Bilateral sudden hearing loss is rarer and more likely to have autoimmune or neurological causes.
Q: Should people with liver disease wear hearing protection at work? A: Yes. Research shows that MASH weakens the cochlea’s resilience to noise trauma [2], so people with metabolic liver disease face higher risk from noise exposure and should use hearing protection proactively.
Conclusion
The emerging link between metabolic liver disease and sudden hearing loss is one of the most practical systemic health connections to understand in 2026. The evidence is clear enough to act on: metabolic dysfunction damages the inner ear through inflammation, vascular injury, and barrier breakdown — and people with MASLD or metabolic syndrome face significantly higher SSNHL risk and worse recovery outcomes.
Actionable next steps:
- If you have MASLD or metabolic syndrome, ask your doctor to include annual hearing screenings in your care plan
- If you experience sudden hearing loss, treat it as an emergency and seek care within 24–72 hours
- Work on metabolic health actively — weight loss, blood sugar control, and exercise protect both your liver and your ears
- Tell your audiologist about your liver health and tell your hepatologist about any hearing changes
- Monitor liver fibrosis markers (FIB-4, APRI) — higher scores may signal elevated cochlear risk [3]
Early awareness of this connection could mean the difference between catching hearing loss before it becomes permanent. Both conditions are manageable — but only if you know to look for them together.
References
[1] PubMed – MASLD and SSNHL risk in older adults – https://pubmed.ncbi.nlm.nih.gov/40352860/
[2] Springer – MASH, cochlear integrity, and blood-labyrinth barrier – https://link.springer.com/article/10.1186/s12964-026-02760-z
[3] PMC – Liver fibrosis indices and SSNHL severity – https://pmc.ncbi.nlm.nih.gov/articles/PMC12423986/
[4] PubMed – Metabolic syndrome and SSNHL meta-analysis – https://pubmed.ncbi.nlm.nih.gov/34325457/
[5] PMC – Metabolic syndrome and poorer SSNHL recovery rates – https://pmc.ncbi.nlm.nih.gov/articles/PMC5876846/
[6] PubMed – Metabolic syndrome as SSNHL risk factor, Taiwan case-control study – https://pubmed.ncbi.nlm.nih.gov/25805640/