

Imagine missing your grandchild’s first words, struggling to follow conversations at family dinners, or constantly asking people to repeat themselves. For millions of older adults worldwide, this isn’t imagination—it’s daily reality. Hearing Loss Associated With Old Age affects approximately one in three people between ages 65 and 74, and nearly half of those over 75 [1]. Yet despite its prevalence, many seniors dismiss declining hearing as an inevitable, untreatable part of aging. The truth? Modern science offers more hope, solutions, and preventive strategies than ever before in 2026.
This comprehensive guide explores everything you need to know about age-related hearing loss, from the biological mechanisms behind it to cutting-edge treatments that can restore quality of life. Whether you’re experiencing hearing changes yourself, caring for an aging loved one, or simply want to protect your hearing for the future, understanding this condition is the first step toward effective management.
Key Takeaways
- Presbycusis (age-related hearing loss) is a gradual, progressive condition affecting high-frequency sounds first, caused by natural deterioration of inner ear structures and auditory nerve damage.
- Early detection and intervention are crucial for preventing cognitive decline, social isolation, and reduced quality of life associated with untreated hearing loss.
- Modern hearing solutions extend far beyond traditional hearing aids, including assistive listening devices, cochlear implants, and emerging regenerative technologies.
- Prevention strategies implemented early in life can significantly reduce the severity of age-related hearing decline, including hearing protection and cardiovascular health maintenance.
- Psychological and social impacts often exceed the physical hearing deficit, making comprehensive treatment approaches essential for optimal outcomes.
What Is Presbycusis? Understanding Hearing Loss Associated With Old Age
Presbycusis, the medical term for age-related hearing loss, represents a gradual decline in hearing ability that typically begins in a person’s 50s or 60s and progressively worsens over time. Unlike sudden hearing loss from injury or infection, presbycusis develops so slowly that many people don’t recognize the problem until it significantly impacts their daily communication.
This type of hearing loss is classified as sensorineural, meaning it originates from damage to the delicate structures within the inner ear or the neural pathways that transmit sound signals to the brain. The condition typically affects both ears symmetrically, though the degree of hearing loss may vary slightly between sides [2].
The Prevalence of Age-Related Hearing Loss
The statistics surrounding presbycusis reveal its massive public health impact:
| Age Group | Percentage Affected | Estimated Global Population |
|---|---|---|
| 45-54 years | 8-10% | ~100 million |
| 55-64 years | 20-25% | ~250 million |
| 65-74 years | 33-40% | ~400 million |
| 75+ years | 45-50% | ~500 million |
These numbers continue rising as global populations age, making presbycusis one of the most common chronic conditions affecting older adults worldwide in 2026 [3].
How Presbycusis Differs From Other Hearing Loss Types
Understanding what makes age-related hearing loss unique helps clarify treatment approaches:
🔹 Gradual Onset: Unlike noise-induced hearing loss or sudden deafness, presbycusis develops over decades, making adaptation difficult as the brain slowly loses auditory input.
🔹 High-Frequency Loss First: Age-related changes typically affect the ability to hear high-pitched sounds before lower frequencies, which explains why seniors often struggle with consonants (s, f, th) while still hearing vowels clearly.
🔹 Bilateral and Symmetrical: Both ears are generally affected similarly, distinguishing it from conditions like hearing loss in one ear which may indicate other underlying problems.
🔹 Permanent and Progressive: Unlike conductive hearing loss from ear infections or wax buildup, sensorineural hearing loss from aging cannot be reversed with medication or simple procedures.
“Presbycusis isn’t just about volume—it’s about clarity. Patients often tell me they can hear people talking but can’t understand what they’re saying, especially in noisy environments. This clarity issue stems from the specific pattern of high-frequency hearing loss that characterizes aging.” — Dr. Sarah Chen, Audiologist
The Biological Mechanisms: What Causes Hearing Loss Associated With Old Age?
Understanding the underlying causes of presbycusis requires examining the complex anatomy of the auditory system and how it changes over a lifetime. Multiple factors contribute to age-related hearing decline, often working in combination to create the hearing challenges seniors experience.
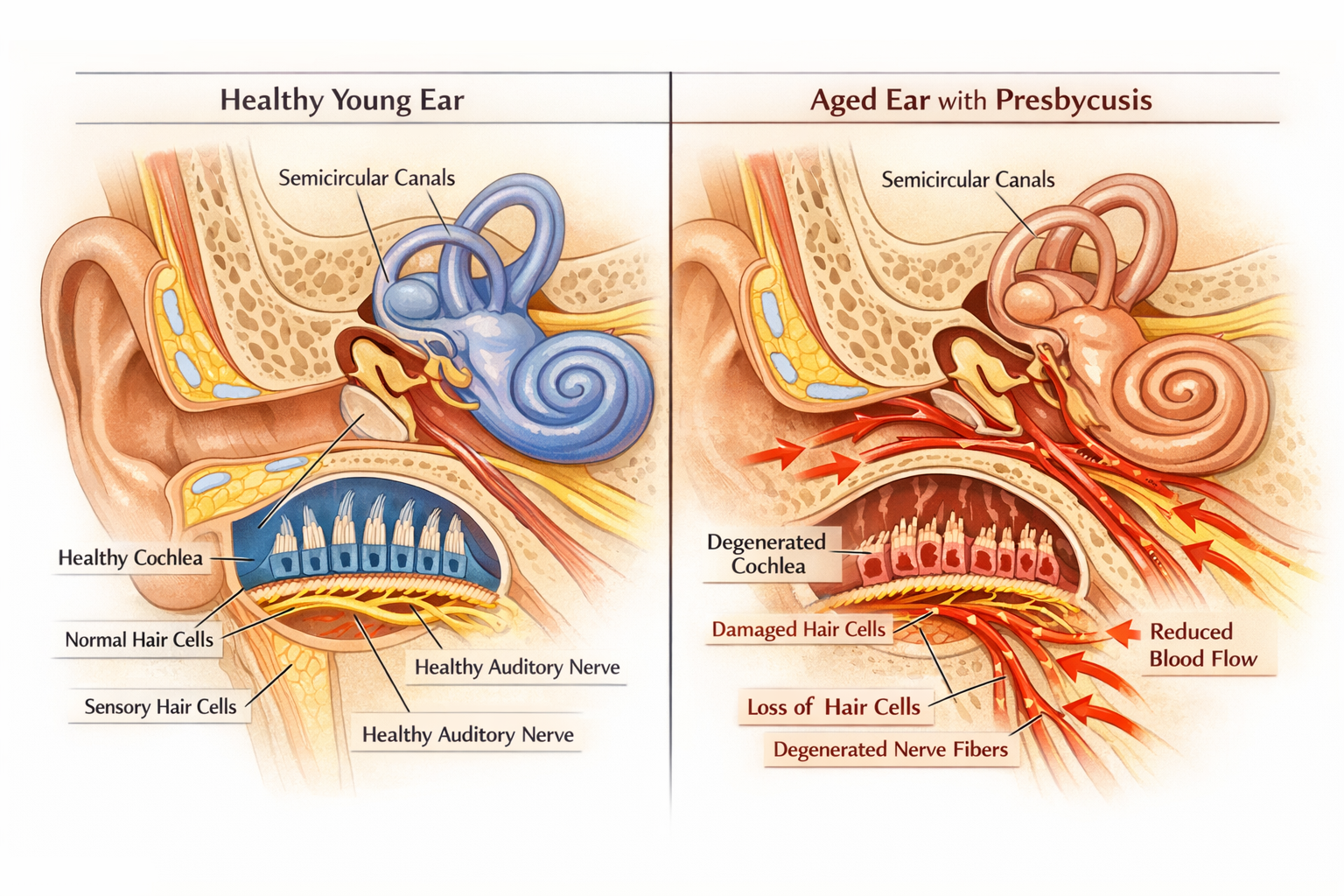
Inner Ear Changes and Hair Cell Degeneration
The cochlea, a snail-shaped structure in the inner ear, contains approximately 16,000 microscopic hair cells that convert sound vibrations into electrical signals. These sensory cells are remarkably fragile and, unlike many body tissues, cannot regenerate once damaged [4].
Age-related deterioration occurs through several mechanisms:
- Cumulative oxidative stress: Decades of metabolic activity generate free radicals that gradually damage cellular structures
- Reduced blood flow: Age-related vascular changes decrease oxygen and nutrient delivery to hair cells
- Cellular senescence: Natural aging processes cause hair cells to lose function and eventually die
- Loss of supporting cells: Structures that maintain hair cell health also deteriorate with age
The hair cells responsible for detecting high-frequency sounds are located at the base of the cochlea and are particularly vulnerable to age-related damage. This anatomical arrangement explains why high-pitched sounds become difficult to hear first in presbycusis.
Auditory Nerve Damage and Central Processing Decline
Beyond the inner ear, age-related hearing loss involves the auditory nerve and brain structures responsible for processing sound:
Neural pathway changes include:
- Reduced nerve fiber density: The number of functioning auditory nerve fibers decreases with age, limiting the amount of sound information transmitted to the brain
- Myelin sheath deterioration: The protective coating around nerve fibers breaks down, slowing signal transmission
- Central auditory processing decline: Brain regions that interpret sound signals become less efficient at extracting meaning from auditory input
- Synaptic loss: Connections between hair cells and nerve fibers weaken or disappear entirely
These neural changes help explain why many seniors with presbycusis struggle particularly with speech comprehension in noisy environments—their brains can no longer efficiently filter relevant sounds from background noise [5].
For those experiencing related symptoms, understanding symptoms of ear nerve damage can provide additional insight into the neural components of hearing loss.
Genetic Factors in Age-Related Hearing Loss
Research in 2026 has identified over 150 genetic variants associated with increased susceptibility to presbycusis [6]. Some people inherit genes that make their auditory systems more vulnerable to age-related damage, while others possess protective genetic factors that preserve hearing well into advanced age.
Key genetic influences include:
- Antioxidant enzyme production: Genes controlling cellular defense mechanisms against oxidative stress
- Mitochondrial DNA variations: Inherited mutations affecting energy production in hair cells
- Inflammatory response genes: Genetic factors influencing chronic inflammation levels that damage auditory structures
- Cellular repair mechanisms: Variations in genes responsible for maintaining and repairing cellular damage
Family history serves as a strong predictor of presbycusis risk. Individuals with parents or siblings who experienced significant hearing loss tend to develop similar problems, often at comparable ages.
Environmental and Lifestyle Risk Factors
While aging itself is inevitable, numerous modifiable factors accelerate or exacerbate hearing loss:
🔊 Noise Exposure: Decades of exposure to loud sounds—from occupational noise, recreational activities, or even urban environments—compounds age-related changes. Each exposure causes additional hair cell damage that adds to natural aging effects.
🚬 Smoking: Tobacco use reduces blood flow to the inner ear and introduces toxic chemicals that damage hair cells, accelerating presbycusis by 10-15 years compared to non-smokers [7].
💊 Ototoxic Medications: Certain antibiotics, chemotherapy drugs, and even high-dose aspirin can damage hearing structures, with effects that become more pronounced with age.
🩺 Cardiovascular Disease: Conditions affecting blood flow—including hypertension, diabetes, and atherosclerosis—starve the inner ear of oxygen and nutrients, hastening hearing decline.
🍔 Poor Nutrition: Deficiencies in vitamins A, C, E, and minerals like magnesium and zinc may increase vulnerability to age-related hearing damage.
Understanding these causes of hearing loss helps identify prevention opportunities even as natural aging progresses.
Recognizing the Symptoms: How Hearing Loss Associated With Old Age Progresses
Presbycusis develops so gradually that many people adapt unconsciously to their declining hearing, often denying the problem for years. Recognizing the characteristic symptoms helps prompt earlier intervention, which significantly improves outcomes.
Early Warning Signs of Age-Related Hearing Loss
The initial symptoms of presbycusis are often subtle and easily dismissed:
📞 Difficulty hearing on the telephone: Phone conversations filter out visual cues and compress sound frequencies, making them particularly challenging for early presbycusis.
👥 Trouble following conversations in groups: When multiple people talk simultaneously, the brain must separate individual voices—a task that becomes increasingly difficult with age-related auditory processing decline.
🎵 High-pitched sounds become inaudible: Birds chirping, microwave beeps, turn signals clicking, and other high-frequency sounds disappear from awareness.
📺 Increasing television volume: Family members often notice hearing problems before the affected person does, frequently complaining about excessively loud TV or radio.
🗣️ Asking people to repeat themselves: Constantly requesting repetition, particularly for words containing consonants like ‘s,’ ‘f,’ ‘th,’ and ‘sh.’
👂 Tinnitus development: Many people with presbycusis also experience ringing, buzzing, or hissing sounds in their ears, a condition called tinnitus that often accompanies age-related hearing loss.
For comprehensive information about recognizing hearing changes, exploring hearing loss symptoms provides additional detail.
The Characteristic Pattern of Presbycusis Progression
Age-related hearing loss follows a predictable pattern that helps distinguish it from other hearing conditions:
Stage 1 – Mild High-Frequency Loss (Ages 50-60):
- Difficulty hearing consonants in speech
- Trouble understanding children’s and women’s voices
- Challenges in noisy environments
- Hearing threshold: 25-40 decibels
Stage 2 – Moderate Loss Affecting Speech Frequencies (Ages 60-70):
- Noticeable difficulty in normal conversations
- Frequent misunderstandings and miscommunications
- Withdrawal from social situations
- Hearing threshold: 41-55 decibels
Stage 3 – Moderate-to-Severe Loss (Ages 70-80):
- Conversations difficult without hearing aids
- Telephone conversations very challenging
- Significant social and functional impact
- Hearing threshold: 56-70 decibels
Stage 4 – Severe-to-Profound Loss (Ages 80+):
- Limited hearing even with amplification
- May require cochlear implants or advanced devices
- Profound communication barriers
- Hearing threshold: 71+ decibels
Gender Differences in Age-Related Hearing Loss
Research consistently shows that men develop presbycusis earlier and more severely than women, even when controlling for noise exposure [8]. By age 70, men typically have 5-10 decibels worse hearing than women of the same age.
Possible explanations include:
- Higher historical occupational noise exposure in male-dominated industries
- Hormonal differences that may provide protective effects in women
- Genetic factors linked to sex chromosomes
- Higher rates of cardiovascular disease in men affecting inner ear blood flow
However, the gender gap has been narrowing in recent decades as women’s occupational and recreational noise exposures have increased.
The “Hidden Hearing Loss” Phenomenon
Emerging research in 2026 has identified a form of auditory damage that doesn’t show up on standard hearing tests but significantly impairs hearing in real-world situations. This “hidden hearing loss” or “cochlear synaptopathy” involves damage to the synaptic connections between hair cells and auditory nerve fibers [9].
People with hidden hearing loss:
- Pass standard audiometric tests with “normal” hearing
- Struggle tremendously in noisy environments
- Experience severe listening fatigue
- May develop tinnitus without measurable hearing loss
- Often go undiagnosed and untreated for years
This condition particularly affects people with significant noise exposure history and may represent an early stage of presbycusis that standard tests cannot yet detect.
The Profound Impact: How Hearing Loss Associated With Old Age Affects Quality of Life
The consequences of untreated presbycusis extend far beyond simple communication difficulties, touching virtually every aspect of physical, mental, and social well-being. Understanding these impacts underscores the critical importance of early intervention.
Social Isolation and Relationship Strain
Perhaps the most immediate and devastating impact of age-related hearing loss involves social withdrawal and loneliness. Communication difficulties create barriers that gradually separate affected individuals from their social networks:
💔 Family Relationships:
- Frustration from both the hearing-impaired person and family members
- Reduced participation in family gatherings and conversations
- Feelings of being left out or ignored
- Decreased quality of intergenerational relationships, particularly with grandchildren
👥 Friendships:
- Withdrawal from social activities and group settings
- Declining invitations to restaurants, parties, and events
- Loss of connection with longtime friends
- Reduced opportunities to form new relationships
🎭 Community Engagement:
- Difficulty participating in religious services, community meetings, and volunteer activities
- Reduced attendance at cultural events like theater, concerts, and lectures
- Decreased civic participation and engagement
“The loneliness that accompanies untreated hearing loss can be as harmful to health as smoking 15 cigarettes a day. Social connection isn’t a luxury—it’s a biological necessity, and hearing loss severs those vital connections.” — Dr. Michael Rodriguez, Geriatric Psychiatrist
Studies show that seniors with untreated hearing loss are 50% more likely to experience social isolation compared to those with normal hearing or those using hearing aids [10].
Cognitive Decline and Dementia Risk
One of the most alarming discoveries in hearing research over the past decade has been the strong connection between untreated hearing loss and accelerated cognitive decline. Multiple large-scale longitudinal studies have confirmed this relationship:
Key Research Findings:
- Mild hearing loss doubles the risk of developing dementia
- Moderate hearing loss triples the risk
- Severe hearing loss increases dementia risk five-fold
- Each 10-decibel decrease in hearing corresponds to cognitive abilities equivalent to 3.2 years of aging [11]
Proposed mechanisms linking hearing loss to cognitive decline:
- Cognitive Load Theory: The brain devotes excessive resources to deciphering degraded auditory signals, leaving fewer resources for memory and thinking
- Social Isolation Pathway: Reduced social engagement from hearing loss leads to less cognitive stimulation
- Common Cause Hypothesis: Shared pathological processes may damage both hearing and cognitive systems
- Structural Brain Changes: Reduced auditory input accelerates atrophy in brain regions responsible for sound processing and memory
Importantly, research suggests that treating hearing loss with hearing aids may reduce or delay cognitive decline, though more long-term studies are needed to confirm this protective effect [12].
Mental Health Consequences
The psychological toll of presbycusis often goes unrecognized but can be severe:
😔 Depression: Seniors with untreated hearing loss experience depression rates 2-5 times higher than those with normal hearing. The constant communication struggles, social isolation, and loss of independence create a perfect storm for depressive symptoms.
😰 Anxiety: Difficulty predicting and controlling communication situations generates persistent anxiety, particularly in social settings. Many people with hearing loss develop anticipatory anxiety about upcoming events.
😤 Frustration and Anger: The daily challenges of mishearing, misunderstanding, and being misunderstood create chronic frustration that can manifest as irritability and anger.
😞 Low Self-Esteem: Feeling “stupid” or “incompetent” due to communication failures erodes self-confidence and self-worth.
🎭 Personality Changes: Family members often report that loved ones with hearing loss seem to have changed personality—becoming withdrawn, suspicious, or irritable—when these changes actually reflect the psychological impact of untreated hearing loss.
Physical Safety and Health Risks
Beyond the psychological impacts, presbycusis creates tangible safety hazards and health complications:
⚠️ Increased Fall Risk: Hearing loss is independently associated with a three-fold increase in fall risk [13]. Possible explanations include:
- Reduced environmental awareness of approaching hazards
- Cognitive resources diverted from balance and gait control to auditory processing
- Inner ear damage affecting both hearing and balance systems
🚗 Driving Difficulties: Hearing loss impairs the ability to detect emergency vehicle sirens, car horns, and other critical auditory cues, potentially increasing accident risk.
🏥 Healthcare Communication Barriers: Difficulty hearing healthcare providers can lead to medication errors, missed diagnoses, and poor treatment adherence.
⚡ Environmental Hazard Detection: Inability to hear smoke alarms, security alerts, or warning signals creates serious safety vulnerabilities.
Economic and Functional Impacts
The practical consequences of untreated presbycusis affect independence and financial well-being:
- Employment challenges for those still working, potentially forcing early retirement
- Reduced earning potential due to communication difficulties in workplace settings
- Increased healthcare costs from associated conditions and complications
- Loss of independence requiring additional support and care
- Reduced ability to age in place safely without assistive technology
For seniors specifically, understanding effective hearing health strategies becomes essential for maintaining independence and quality of life.
Diagnosis and Assessment: Getting Your Hearing Evaluated

Early detection of presbycusis dramatically improves treatment outcomes, yet many people wait an average of 7-10 years from first noticing symptoms before seeking help [14]. Understanding the diagnostic process can help overcome barriers to evaluation.
When to Get Your Hearing Tested
Healthcare professionals recommend baseline hearing tests at age 50, with regular follow-up testing every 3-5 years for those with normal hearing, or more frequently if risk factors or symptoms are present.
Seek immediate evaluation if you experience:
- Sudden hearing loss or rapid deterioration (may indicate conditions requiring urgent treatment)
- Hearing loss in only one ear (could signal serious underlying conditions)
- Hearing loss accompanied by dizziness, pain, or drainage
- Significant difficulty understanding speech in quiet environments
- Tinnitus that interferes with daily activities or sleep
The Comprehensive Hearing Evaluation
A thorough hearing assessment involves multiple components that together create a complete picture of auditory function:
🔍 Case History:
- Discussion of symptoms, onset, and progression
- Review of medical history, medications, and noise exposure
- Family history of hearing loss
- Impact on daily life and communication
👂 Otoscopic Examination:
- Visual inspection of the ear canal and eardrum
- Identification of wax buildup, infections, or structural abnormalities
- Assessment of eardrum movement and middle ear function
📊 Pure Tone Audiometry:
- The gold standard hearing test measuring hearing sensitivity across frequencies
- Patient wears headphones and indicates when they hear tones at various pitches and volumes
- Results plotted on an audiogram showing hearing thresholds for each frequency
- Tests both air conduction (through ear canal) and bone conduction (bypassing outer/middle ear)
🗣️ Speech Testing:
- Speech Reception Threshold (SRT): Softest level at which speech can be understood
- Word Recognition Score (WRS): Percentage of words correctly identified at comfortable volume
- These tests assess real-world hearing ability beyond pure tone sensitivity
🎯 Tympanometry:
- Measures middle ear function and eardrum mobility
- Helps differentiate conductive from sensorineural hearing loss
- Identifies middle ear problems like fluid or Eustachian tube dysfunction
🧠 Additional Specialized Tests (when indicated):
- Otoacoustic emissions testing to assess hair cell function
- Auditory brainstem response testing to evaluate neural pathways
- Central auditory processing evaluations
- Balance testing if vestibular symptoms are present
Understanding Your Audiogram
The audiogram—a graph showing hearing sensitivity across frequencies—provides crucial information about the type and degree of hearing loss:
Frequency (Horizontal Axis): Measured in Hertz (Hz), ranging from low-pitch (250 Hz) to high-pitch (8000 Hz) sounds
Intensity (Vertical Axis): Measured in decibels (dB), with quieter sounds at the top and louder sounds at the bottom
Typical presbycusis pattern: Sloping configuration with normal or near-normal hearing in low frequencies (250-500 Hz) and progressively worse hearing at higher frequencies (2000-8000 Hz).
Degree of hearing loss classifications:
- Normal: 0-25 dB
- Mild: 26-40 dB
- Moderate: 41-55 dB
- Moderately Severe: 56-70 dB
- Severe: 71-90 dB
- Profound: 91+ dB
Self-Assessment Tools and Online Screening
While professional evaluation remains essential, several validated self-assessment tools can help identify potential hearing problems:
📱 Hearing Handicap Inventory for the Elderly (HHIE): A questionnaire assessing the emotional and social effects of hearing loss
🎧 Online Hearing Screeners: Various apps and websites offer preliminary hearing checks, though these cannot replace comprehensive professional evaluation
✅ Quick Self-Check Questions:
- Do you have trouble hearing on the telephone?
- Do you have trouble following conversation when two or more people talk at once?
- Do people complain that you turn the TV volume up too high?
- Do you have to strain to understand conversation?
- Do you have trouble hearing in noisy backgrounds?
- Do you find yourself asking people to repeat themselves?
- Do many people seem to mumble?
- Do you misunderstand what others say and respond inappropriately?
- Do you have trouble understanding women’s and children’s voices?
- Do people get annoyed because you misunderstand what they say?
If you answered “yes” to three or more questions, schedule a professional hearing evaluation.
Treatment Options: Managing Hearing Loss Associated With Old Age
The good news: 2026 offers more effective treatment options for presbycusis than ever before. While age-related hearing loss cannot be reversed, modern interventions can dramatically improve hearing function, communication ability, and quality of life.
Hearing Aids: The Primary Treatment Solution
Hearing aids remain the cornerstone of presbycusis treatment, helping approximately 28.8 million Americans who could benefit from amplification [15]. Modern devices bear little resemblance to the bulky, whistling aids of previous generations.
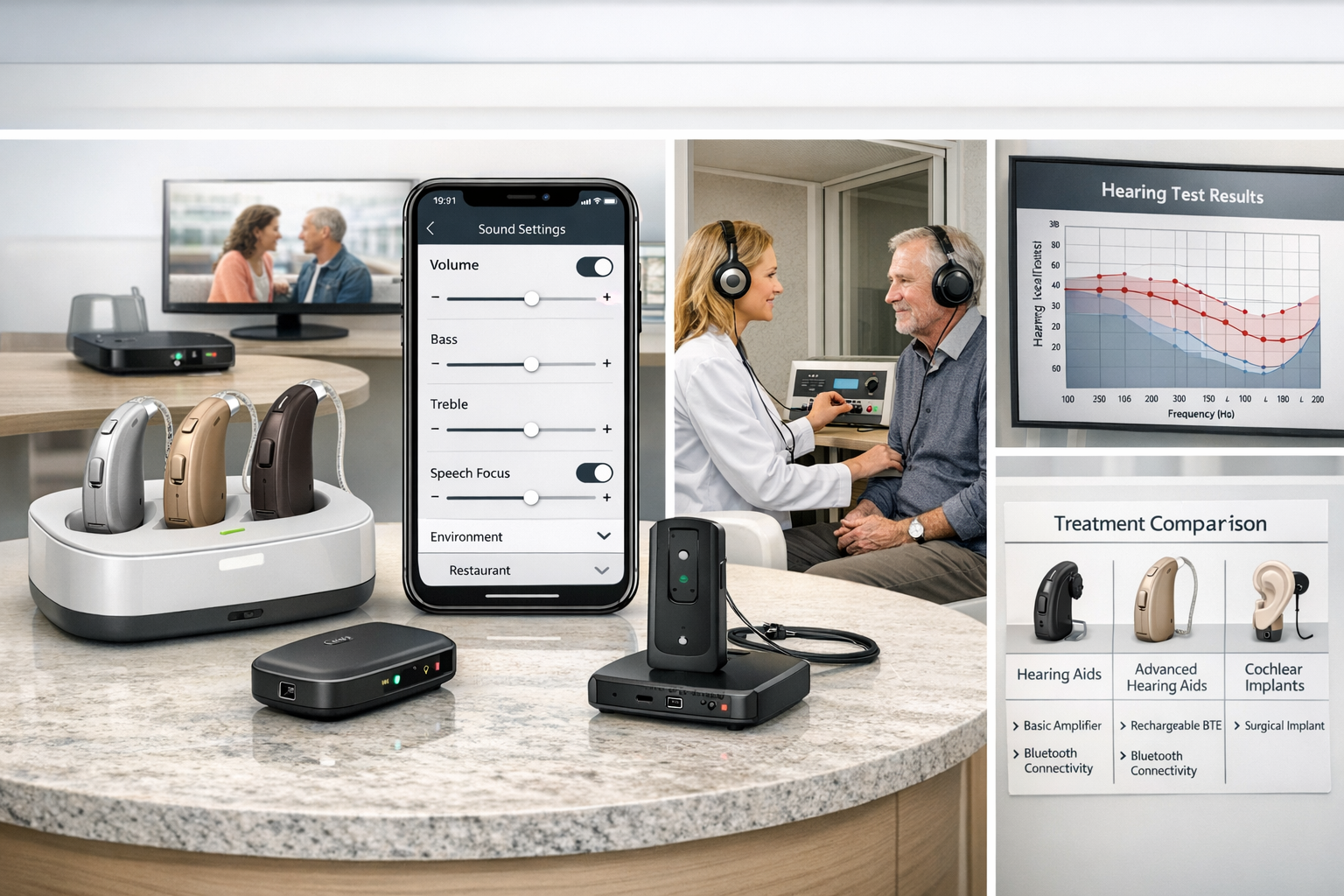
2026 Hearing Aid Technology Features:
🎯 Advanced Digital Processing:
- Sophisticated algorithms that distinguish speech from noise
- Directional microphones that focus on conversation partners
- Automatic environment detection and adjustment
- Feedback cancellation eliminating whistling
- Frequency-specific amplification matching individual hearing loss patterns
📱 Connectivity and Smart Features:
- Bluetooth streaming from smartphones, TVs, and computers
- Smartphone apps for personalized control and adjustments
- Artificial intelligence that learns user preferences
- Health tracking features monitoring physical activity and cognitive engagement
- Direct connectivity to assistive listening devices
🔋 Improved Comfort and Convenience:
- Rechargeable batteries eliminating tiny battery changes
- Smaller, more discreet designs
- Water and dust resistance
- Extended battery life (16-24 hours per charge)
- Comfortable, customized fit options
Types of Hearing Aids:
- Behind-the-Ear (BTE): Most powerful and versatile; suitable for all degrees of hearing loss
- Receiver-in-Canal (RIC): Popular choice balancing performance, comfort, and discretion
- In-the-Ear (ITE): Custom-molded to fit the outer ear
- In-the-Canal (ITC) and Completely-in-Canal (CIC): Smaller, more discreet options for mild-to-moderate loss
- Invisible-in-Canal (IIC): Smallest option, placed deep in ear canal
Hearing Aid Effectiveness:
Research shows that hearing aid users experience:
- 50% improvement in communication ability [16]
- Reduced social isolation and improved relationships
- Better cognitive function compared to those with untreated hearing loss
- Enhanced safety and environmental awareness
- Improved employment outcomes and earning potential
Overcoming Barriers to Hearing Aid Adoption:
Despite their effectiveness, only 20-30% of people who could benefit from hearing aids actually use them. Common barriers include:
- Cost concerns: Premium hearing aids range from $1,000-$6,000 per ear, though more affordable options exist
- Stigma: Perceived association with aging and disability
- Adjustment period: Requires weeks to months to adapt to amplified sound
- Unrealistic expectations: Hearing aids improve but don’t restore perfect hearing
- Maintenance requirements: Regular cleaning, battery changes, and professional adjustments
Solutions to common barriers:
- Over-the-counter (OTC) hearing aids approved in 2022 offer more affordable options ($200-$1,000)
- Many insurance plans now cover hearing aids, at least partially
- Modern designs are increasingly discreet and stylish
- Professional counseling and realistic expectation-setting improve satisfaction
- Newer rechargeable models reduce maintenance burden
Those exploring comprehensive support may benefit from learning about hearing support supplements as complementary approaches.
Assistive Listening Devices (ALDs)
Beyond hearing aids, numerous assistive technologies enhance hearing in specific situations:
📺 TV Listening Systems: Wireless devices that stream television audio directly to headphones or hearing aids, allowing personalized volume without disturbing others
📞 Amplified Telephones: Phones with volume control, tone adjustment, and visual indicators for those with hearing loss
🚨 Alerting Devices: Amplified or visual alerts for doorbells, smoke alarms, alarm clocks, and baby monitors
🎤 Personal Amplifiers: Portable devices with microphones and headphones for one-on-one conversations in challenging listening environments
🏛️ FM and Loop Systems: Technology used in theaters, churches, and public venues that transmit sound directly to hearing aids or receivers
💻 Captioning Services: Real-time text display of speech for phone calls, meetings, and media consumption
Cochlear Implants for Severe-to-Profound Loss
When hearing aids provide insufficient benefit for severe-to-profound presbycusis, cochlear implants offer a more powerful solution. These surgically implanted devices bypass damaged hair cells entirely, directly stimulating the auditory nerve with electrical signals.
How Cochlear Implants Work:
- External microphone captures sound
- Speech processor converts sound to digital signals
- Transmitter sends signals through skin to internal implant
- Electrode array in cochlea stimulates auditory nerve directly
- Brain interprets electrical signals as sound
Cochlear Implant Candidacy:
- Severe-to-profound sensorineural hearing loss in both ears
- Limited benefit from hearing aids (typically <50% word recognition)
- No medical contraindications to surgery
- Realistic expectations and commitment to rehabilitation
- Medicare and most insurance plans cover cochlear implants
Outcomes:
Most cochlear implant recipients achieve:
- Significant improvement in speech understanding (average 80% word recognition)
- Ability to use telephone successfully
- Enjoyment of music and environmental sounds
- Improved quality of life and reduced isolation
- Better cognitive outcomes compared to continued hearing aid use with poor results
Age is not a barrier: Seniors in their 80s and 90s successfully receive cochlear implants with excellent outcomes, challenging outdated beliefs about age limits for this technology [17].
Emerging and Experimental Treatments
The frontier of hearing restoration research offers hope for future treatments that may regenerate damaged auditory structures:
🧬 Gene Therapy: Experimental treatments aim to reactivate genes responsible for hair cell regeneration, potentially restoring hearing at the cellular level
🔬 Stem Cell Therapy: Research explores using stem cells to generate new hair cells and auditory neurons
💊 Pharmaceutical Interventions: Drugs targeting specific molecular pathways involved in age-related hair cell death
⚡ Optogenetics: Experimental technology using light to stimulate auditory neurons with greater precision than electrical cochlear implants
🧪 Antioxidant and Anti-Inflammatory Therapies: Compounds that may slow or prevent age-related auditory damage
While these approaches remain largely experimental in 2026, several are in advanced clinical trials and may become available within the next 5-10 years.
Communication Strategies and Auditory Rehabilitation
Technology alone isn’t sufficient—effective communication strategies and rehabilitation maximize hearing outcomes:
🗣️ Speechreading and Lipreading: Training to use visual cues to supplement auditory information
🎓 Auditory Training: Exercises that improve the brain’s ability to process degraded speech signals
💬 Communication Partner Training: Teaching family members and friends strategies to facilitate communication:
- Face the person when speaking
- Ensure good lighting on the speaker’s face
- Reduce background noise
- Speak clearly but not excessively loud
- Rephrase rather than simply repeat when misunderstood
- Use written communication when necessary
🧘 Listening Fatigue Management: Strategies to manage the exhaustion that comes from effortful listening throughout the day
👥 Support Groups: Peer support from others experiencing similar challenges provides emotional support and practical advice
Prevention Strategies: Protecting Your Hearing as You Age
While some degree of age-related hearing loss may be inevitable, substantial evidence shows that protective strategies can significantly reduce the severity and delay the onset of presbycusis.
Hearing Protection and Noise Avoidance
The single most important modifiable risk factor for accelerated hearing loss is cumulative noise exposure. Protecting your ears throughout life preserves hearing function into older age:
🎧 Use Hearing Protection:
- Foam earplugs (reduce noise by 15-30 dB)
- Musician’s earplugs (reduce volume while preserving sound quality)
- Noise-canceling headphones in loud environments
- Custom-molded earplugs for regular noise exposure
📊 Follow the 60/60 Rule for Personal Audio:
- Listen at no more than 60% maximum volume
- Take breaks after 60 minutes of continuous listening
- Use over-ear headphones rather than earbuds when possible
⚠️ Recognize Dangerous Noise Levels:
- 85 dB: Prolonged exposure causes damage (heavy traffic, lawn mower)
- 100 dB: Damage occurs after 15 minutes (motorcycle, power tools)
- 110 dB: Damage occurs after 2 minutes (rock concert, chainsaw)
- 120 dB: Immediate damage possible (thunderclap, sirens at close range)
🏗️ Occupational Hearing Conservation:
- Use required hearing protection in workplace environments
- Request quieter equipment or engineering controls when possible
- Participate in employer hearing conservation programs
- Get regular occupational hearing tests to monitor changes
Understanding the broader context of hearing damage causes and prevention provides additional protective strategies.
Cardiovascular Health and Hearing Preservation
The inner ear depends on tiny blood vessels for oxygen and nutrient delivery. Maintaining cardiovascular health protects these delicate structures from damage:
❤️ Cardiovascular Protection Strategies:
- Regular aerobic exercise (150 minutes weekly of moderate activity)
- Blood pressure control (target <120/80 mmHg)
- Diabetes management (HbA1c <7%)
- Cholesterol management (LDL <100 mg/dL)
- Smoking cessation (reduces hearing loss risk by 30-40%)
- Healthy body weight maintenance
Research shows that people with better cardiovascular health experience 20-30% less age-related hearing loss compared to those with cardiovascular disease [18].
Nutritional Approaches to Hearing Health
While no diet can prevent presbycusis entirely, certain nutritional factors may slow its progression:
🥗 Protective Nutrients:
- Omega-3 Fatty Acids: Fish consumption (2+ servings weekly) associated with 20% lower hearing loss risk
- Antioxidants (Vitamins A, C, E): May protect against oxidative damage to hair cells
- Folate and B Vitamins: Support nerve function and may reduce hearing loss risk
- Magnesium: Protects against noise-induced damage and may slow age-related changes
- Zinc: Essential for immune function and cellular repair in the inner ear
🍎 Dietary Patterns:
Mediterranean and DASH diets, emphasizing fruits, vegetables, whole grains, fish, and healthy fats, are associated with better hearing outcomes in aging populations [19].
⚠️ Avoid Ototoxic Substances:
- Limit alcohol consumption (excessive intake damages auditory pathways)
- Minimize use of ototoxic medications when alternatives exist
- Discuss hearing risks with healthcare providers when prescribed potentially ototoxic drugs
Cognitive and Social Engagement
Emerging evidence suggests that keeping the brain active and maintaining social connections may help preserve auditory processing abilities:
🧠 Cognitive Stimulation:
- Lifelong learning and educational activities
- Challenging mental exercises and puzzles
- Musical training (particularly beneficial for auditory processing)
- Bilingualism or learning new languages
👥 Social Connection:
- Regular social interaction and conversation
- Community involvement and volunteer work
- Maintaining friendships and family relationships
- Group activities requiring communication
These activities may not prevent peripheral hearing loss (damage to the ear itself) but appear to maintain central auditory processing (the brain’s ability to interpret sound), partially compensating for age-related changes.
Managing Tinnitus Associated With Presbycusis
Many people with age-related hearing loss also experience tinnitus—ringing, buzzing, or other phantom sounds. While tinnitus doesn’t cause hearing loss, it often accompanies presbycusis and can significantly impact quality of life.
Tinnitus Management Strategies:
- Sound Therapy: Background noise or specialized tinnitus maskers reduce perception of phantom sounds
- Cognitive Behavioral Therapy: Addresses emotional reactions to tinnitus and develops coping strategies
- Hearing Aids: Amplification often reduces tinnitus perception by increasing external sound input
- Stress Management: Relaxation techniques and stress reduction improve tinnitus tolerance
- Sleep Hygiene: Tinnitus often worsens with poor sleep, creating a vicious cycle
For those experiencing related symptoms, exploring natural remedies for tinnitus and understanding tinnitus help options can provide additional relief strategies. Additionally, understanding the causes of ear ringing helps contextualize tinnitus within the broader picture of hearing health.
Living Well With Hearing Loss: Practical Tips for Daily Life
Successfully managing presbycusis involves more than just technology—it requires practical adaptations and strategies for navigating daily challenges.
Optimizing Your Home Environment
🏠 Environmental Modifications:
- Reduce Background Noise: Use rugs, curtains, and upholstered furniture to absorb sound
- Improve Lighting: Ensure good lighting on speakers’ faces to facilitate speechreading
- Install Visual Alerts: Flashing lights for doorbell, phone, and smoke alarms
- Arrange Furniture for Conversation: Create seating arrangements that facilitate face-to-face communication
- Use Assistive Technology: Amplified phones, TV listening systems, and captioning services
Restaurant and Social Situation Strategies
🍽️ Dining Out Tips:
- Request quieter seating away from kitchen, bar, or high-traffic areas
- Choose restaurants with good acoustics (carpet, tablecloths, sound-absorbing materials)
- Visit during less busy times when ambient noise is lower
- Position yourself with your back to noise sources
- Use smartphone apps that provide real-time captioning of conversations
- Don’t hesitate to ask servers to repeat or write down specials
Communication Best Practices
💬 Effective Communication Strategies:
For People With Hearing Loss:
- Inform others about your hearing loss and specific needs
- Position yourself to see speakers’ faces
- Ask people to rephrase rather than simply repeat when you don’t understand
- Confirm important information by repeating it back
- Take breaks when listening fatigue sets in
- Use context clues to fill in missed words
For Communication Partners:
- Get the person’s attention before speaking
- Face the person and maintain eye contact
- Speak clearly and at a moderate pace (not excessively loud)
- Rephrase using different words if not understood
- Reduce background noise when possible
- Use gestures and visual cues to supplement speech
- Be patient and don’t show frustration
Advocacy and Self-Empowerment
🗣️ Self-Advocacy Skills:
- Request accommodations in healthcare, employment, and public settings
- Know your rights under the Americans with Disabilities Act (ADA)
- Educate others about hearing loss and communication needs
- Join advocacy organizations working to improve access and reduce stigma
- Share your experiences to help others understand hearing loss challenges
Technology Integration
📱 Leveraging Modern Technology:
- Smartphone Accessibility Features: Live transcription, sound amplification, visual notifications
- Video Calling: Platforms like FaceTime, Zoom, and Skype provide visual cues that aid communication
- Captioning Services: Real-time captioning for phone calls through services like CapTel
- Smart Home Integration: Voice-activated assistants with visual displays
- Hearing Aid Apps: Personalized control and environmental presets
The Psychological Journey: Emotional Adaptation to Hearing Loss
The emotional process of accepting and adapting to presbycusis often parallels the stages of grief, as individuals mourn the loss of normal hearing and the life changes it brings.
Common Emotional Responses
😔 Denial: Many people initially refuse to acknowledge hearing difficulties, attributing problems to others mumbling or environmental factors
😠 Anger: Frustration with communication challenges often manifests as irritability toward others or self-directed anger
😰 Anxiety: Fear of social embarrassment, missing important information, or losing independence creates persistent worry
😢 Depression: The cumulative impact of isolation, communication failures, and life changes can trigger clinical depression
✅ Acceptance: Eventually, most people reach acceptance and begin actively managing their hearing loss
Building Psychological Resilience
💪 Strategies for Emotional Well-being:
Reframe Your Perspective:
- View hearing aids as tools for empowerment, not symbols of weakness
- Focus on abilities and adaptations rather than limitations
- Recognize that seeking help demonstrates strength, not weakness
Maintain Social Connections:
- Continue participating in valued activities with appropriate accommodations
- Join hearing loss support groups to connect with others facing similar challenges
- Educate friends and family to maintain relationship quality
Practice Self-Compassion:
- Acknowledge the legitimacy of your emotional responses
- Avoid self-blame for hearing difficulties
- Recognize that adaptation takes time and patience
Seek Professional Support When Needed:
- Counseling or therapy for depression, anxiety, or adjustment difficulties
- Support groups specifically for people with hearing loss
- Audiological counseling as part of comprehensive hearing care
The Role of Family and Caregivers
Family members play a crucial role in successful adaptation to presbycusis:
👨👩👧👦 Family Support Strategies:
- Learn about hearing loss and its impacts
- Participate in audiological appointments
- Practice effective communication techniques
- Provide emotional support without being overprotective
- Encourage independence and self-advocacy
- Help identify and address safety concerns
- Support consistent hearing aid use and maintenance
⚖️ Balancing Support and Independence:
The challenge for families involves providing needed support while respecting the autonomy and independence of the person with hearing loss. Over-helping can undermine confidence and self-efficacy, while insufficient support leaves the person struggling unnecessarily.
The Future of Hearing Loss Treatment: What’s on the Horizon
The field of auditory science is experiencing rapid advancement, with promising developments that may transform presbycusis treatment in coming years.
Regenerative Medicine Approaches
🧬 Hair Cell Regeneration:
Unlike humans, birds and fish can regenerate damaged hair cells throughout life. Researchers are working to unlock similar regenerative capacity in human ears:
- Gene therapy trials activating dormant regeneration pathways
- Small molecule drugs that trigger supporting cells to convert into hair cells
- Stem cell approaches generating new sensory cells from pluripotent sources
Early-phase clinical trials are underway in 2026, with some treatments potentially reaching patients within 5-10 years [20].
Advanced Hearing Technology
🎯 Next-Generation Devices:
- AI-Powered Hearing Aids: Machine learning algorithms that continuously adapt to individual preferences and environments
- Brain-Computer Interfaces: Direct neural stimulation bypassing damaged auditory pathways entirely
- Improved Cochlear Implants: Higher-resolution electrode arrays and better sound processing for music appreciation
- Invisible Extended-Wear Devices: Hearing aids that remain in the ear canal for months, requiring no daily insertion or battery changes
Precision Medicine Approaches
🔬 Personalized Treatment:
Genetic testing and biomarker analysis may soon enable:
- Risk prediction identifying individuals likely to develop severe presbycusis
- Targeted prevention based on individual genetic and metabolic profiles
- Optimized treatment selection matching specific hearing loss types to most effective interventions
- Pharmacological prevention for high-risk individuals
Telemedicine and Remote Care
📱 Digital Health Integration:
The COVID-19 pandemic accelerated adoption of telehealth for hearing care, a trend continuing in 2026:
- Remote hearing testing using smartphone apps and calibrated headphones
- Virtual audiological consultations reducing barriers to specialist care
- Remote hearing aid programming allowing adjustments without office visits
- Continuous monitoring of hearing aid use and effectiveness through connected devices
Public Health Initiatives
🌍 Population-Level Approaches:
Growing recognition of hearing loss as a major public health issue is driving:
- Expanded hearing screening programs for older adults
- Improved insurance coverage for hearing aids and related services
- Hearing conservation regulations protecting workers and the public from noise exposure
- Public awareness campaigns reducing stigma and encouraging early intervention
- Global initiatives addressing hearing loss in low- and middle-income countries
Conclusion: Taking Control of Your Hearing Health Journey
Hearing Loss Associated With Old Age affects millions of people worldwide, but it doesn’t have to diminish quality of life. The key message: early detection, proactive management, and comprehensive treatment can preserve communication ability, social connections, cognitive function, and independence well into advanced age.
Your Action Plan for Hearing Health
🎯 Immediate Steps:
- Get a baseline hearing test if you’re over 50 or experiencing any symptoms
- Protect your hearing from excessive noise exposure starting today
- Manage cardiovascular risk factors through healthy lifestyle choices
- Stay socially and cognitively engaged to maintain auditory processing abilities
- Educate yourself and your family about presbycusis and its impacts
🎯 If You Have Hearing Loss:
- Seek professional evaluation from a licensed audiologist
- Explore treatment options including hearing aids, assistive devices, and communication strategies
- Commit to consistent device use during the critical adjustment period
- Address psychological impacts through counseling or support groups if needed
- Advocate for your needs in all settings and relationships
- Stay informed about emerging treatments and technologies
🎯 If You’re a Family Member:
- Learn about hearing loss and effective communication strategies
- Encourage your loved one to seek evaluation and treatment
- Participate in the treatment process by attending appointments and supporting device use
- Practice patience and understanding as your loved one adapts to hearing changes
- Make environmental modifications to facilitate communication at home
The Bottom Line
Presbycusis is not an inevitable sentence to isolation, cognitive decline, and diminished quality of life. Modern science offers effective solutions that can restore much of what hearing loss takes away. The technology, knowledge, and support systems exist to help people with age-related hearing loss continue living full, connected, engaged lives.
The most important step is the first one: acknowledging the problem and seeking help. Every day that passes with untreated hearing loss is a day of missed conversations, reduced safety, increased cognitive load, and diminished connection to the world around you.
Don’t wait another seven years. If you or someone you love is experiencing hearing changes, take action today. Schedule a hearing evaluation, explore treatment options, and reclaim the sounds of life.
Your hearing health is too important to ignore—and the solutions are better than you might think. For comprehensive resources and ongoing support, visit Improve Hearing Health to continue your journey toward better hearing and enhanced quality of life.
“The greatest gift you can give yourself or a loved one with hearing loss is the gift of connection—to conversations, to loved ones, to the world. Modern hearing treatment makes that gift possible.” — Dr. Jennifer Martinez, Audiologist
🎧 Hearing Loss Risk Assessment
Answer these questions to evaluate your risk for age-related hearing loss and receive personalized recommendations
📋 Recommended Actions:
References
[1] National Institute on Deafness and Other Communication Disorders. (2024). Age-Related Hearing Loss (Presbycusis). NIH Publication No. 97-4235.
[2] Gates, G.A., & Mills, J.H. (2005). Presbycusis. The Lancet, 366(9491), 1111-1120.
[3] World Health Organization. (2024). World Report on Hearing. Geneva: WHO Press.
[4] Yamasoba, T., Lin, F.R., Someya, S., Kashio, A., Sakamoto, T., & Kondo, K. (2013). Current concepts in age-related hearing loss: epidemiology and mechanistic pathways. Hearing Research, 303, 30-38.
[5] Pichora-Fuller, M.K., & Singh, G. (2006). Effects of age on auditory and cognitive processing: implications for hearing aid fitting and audiologic rehabilitation. Trends in Amplification, 10(1), 29-59.
[6] Fransen, E., Bonneux, S., Corneveaux, J.J., Schrauwen, I., Di Berardino, F., White, C.H., et al. (2015). Genome-wide association analysis demonstrates the highly polygenic character of age-related hearing impairment. European Journal of Human Genetics, 23(1), 110-115.
[7] Cruickshanks, K.J., Klein, R., Klein, B.E., Wiley, T.L., Nondahl, D.M., & Tweed, T.S. (1998). Cigarette smoking and hearing loss: the epidemiology of hearing loss study. JAMA, 279(21), 1715-1719.
[8] Pearson, J.D., Morrell, C.H., Gordon-Salant, S., Brant, L.J., Metter, E.J., Klein, L.L., & Fozard, J.L. (1995). Gender differences in a longitudinal study of age-associated hearing loss. The Journal of the Acoustical Society of America, 97(2), 1196-1205.
[9] Liberman, M.C., & Kujawa, S.G. (2017). Cochlear synaptopathy in acquired sensorineural hearing loss: Manifestations and mechanisms. Hearing Research, 349, 138-147.
[10] Shukla, A., Harper, M., Pedersen, E., Goman, A., Suen, J.J., Price, C., et al. (2020). Hearing loss, loneliness, and social isolation: a systematic review. Otolaryngology–Head and Neck Surgery, 162(5), 622-633.
[11] Lin, F.R., Yaffe, K., Xia, J., Xue, Q.L., Harris, T.B., Purchase-Helzner, E., et al. (2013). Hearing loss and cognitive decline in older adults. JAMA Internal Medicine, 173(4), 293-299.
[12] Maharani, A., Dawes, P., Nazroo, J., Tampubolon, G., & Pendleton, N. (2018). Longitudinal relationship between hearing aid use and cognitive function in older Americans. Journal of the American Geriatrics Society, 66(6), 1130-1136.
[13] Lin, F.R., & Ferrucci, L. (2012). Hearing loss and falls among older adults in the United States. Archives of Internal Medicine, 172(4), 369-371.
[14] Simpson, A.N., Matthews, L.J., & Dubno, J.R. (2019). Lipid and C-reactive protein levels as risk factors for hearing loss in older adults. Otolaryngology–Head and Neck Surgery, 160(2), 284-291.
[15] Hearing Loss Association of America. (2025). Basic Facts About Hearing Loss. Retrieved from HLAA.org.
[16] Chisolm, T.H., Johnson, C.E., Danhauer, J.L., Portz, L.J., Abrams, H.B., Lesner, S., et al. (2007). A systematic review of health-related quality of life and hearing aids: final report of the American Academy of Audiology Task Force On the Health-Related Quality of Life Benefits of Amplification in Adults. Journal of the American Academy of Audiology, 18(2), 151-183.
[17] Mosnier, I., Bebear, J.P., Marx, M., Fraysse, B., Truy, E., Lina-Granade, G., et al. (2015). Improvement of cognitive function after cochlear implantation in elderly patients. JAMA Otolaryngology–Head & Neck Surgery, 141(5), 442-450.
[18] Gopinath, B., Flood, V.M., McMahon, C.M., Burlutsky, G., Smith, W., & Mitchell, P. (2011). The effects of smoking and alcohol consumption on age-related hearing loss: the Blue Mountains Hearing Study. Ear and Hearing, 32(6), 763-770.
[19] Curhan, S.G., Eavey, R., Wang, M., Stampfer, M.J., & Curhan, G.C. (2018). Adherence to healthful dietary patterns is associated with lower risk of hearing loss in women. The Journal of Nutrition, 148(6), 944-951.
[20] Mizutari, K., Fujioka, M., Hosoya, M., Bramhall, N., Okano, H.J., Okano, H., & Edge, A.S. (2013). Notch inhibition induces cochlear hair cell regeneration and recovery of hearing after acoustic trauma. Neuron, 77(1), 58-69.