
Understanding Ear Disorders That Cause Dizziness: A Complete Guide to Balance Problems
Have you ever stood up too quickly and felt the room spin around you? Or perhaps you’ve experienced a sudden wave of dizziness that made you grab onto the nearest wall for support? While occasional lightheadedness happens to everyone, persistent or severe dizziness often points to something more serious—specifically, ear disorders that cause dizziness. Your ears do more than help you hear; they’re essential for maintaining balance and spatial orientation. When something goes wrong in the delicate structures of your inner ear, the result can be debilitating vertigo, constant unsteadiness, and a significant impact on your quality of life.
Key Takeaways
- The inner ear controls both hearing and balance through specialized structures called the vestibular system, which is why ear problems often cause dizziness
- BPPV (Benign Paroxysmal Positional Vertigo) is the most common ear disorder causing dizziness, affecting millions of people and characterized by brief spinning sensations triggered by head movements
- Meniere’s disease, vestibular neuritis, and labyrinthitis are other major ear-related conditions that can cause severe vertigo, hearing loss, and balance problems
- Early diagnosis and treatment are crucial for managing symptoms and preventing complications, with options ranging from simple repositioning maneuvers to medications and therapy
- Most ear disorders that cause dizziness are treatable, and many people experience significant improvement with proper medical care and lifestyle modifications
What Are Ear Disorders That Cause Dizziness? 🏥
Ear disorders that cause dizziness are medical conditions affecting the inner ear’s vestibular system—the complex network of structures responsible for maintaining your sense of balance and spatial orientation. These conditions disrupt the normal signals sent from your inner ear to your brain, creating a mismatch between what your eyes see and what your balance system feels.
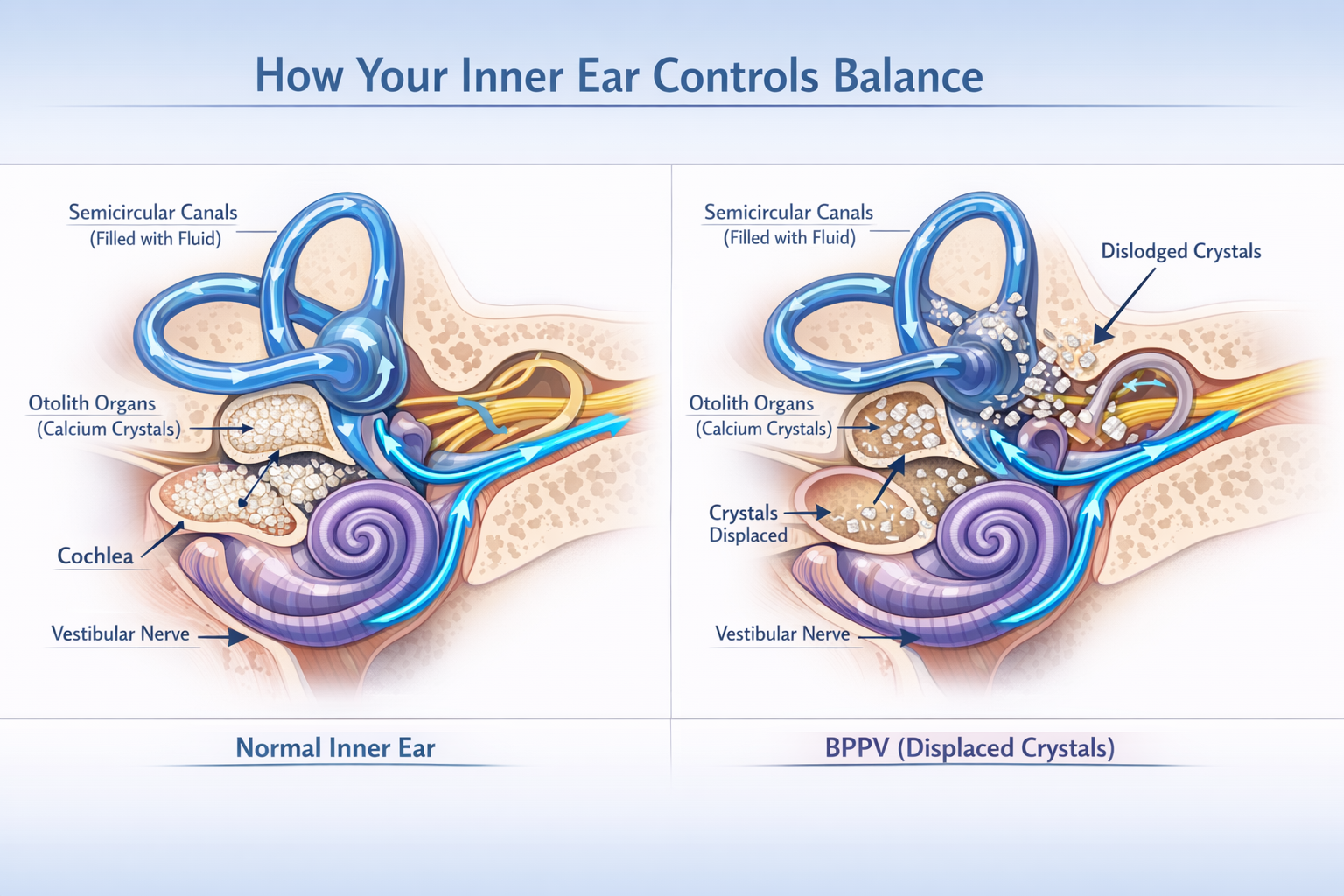
The vestibular system consists of three semicircular canals filled with fluid and tiny hair cells that detect head movements, along with two organs called the utricle and saccule that sense gravity and linear acceleration. When these structures become damaged, inflamed, or dysfunctional, they send incorrect information to your brain about your body’s position in space.
The Connection Between Your Ears and Balance
Most people don’t realize that their ears play such a critical role in balance. Here’s how it works:
- Fluid movement: When you move your head, fluid in the semicircular canals shifts, bending tiny hair cells
- Signal transmission: These hair cells convert mechanical movement into electrical signals
- Brain processing: Your brain receives these signals and combines them with visual and proprioceptive (body position) information
- Balance coordination: Your brain uses all this data to maintain equilibrium and coordinate movement
When any part of this system malfunctions, you experience dizziness, vertigo, or imbalance. Understanding hearing loss symptoms can help you recognize when ear problems might be affecting your balance as well.
Common Ear Disorders That Cause Dizziness and Vertigo
Let’s explore the most prevalent ear conditions that lead to dizziness, their unique characteristics, and what makes each one distinct.
Benign Paroxysmal Positional Vertigo (BPPV) 🌀
BPPV is the most common cause of vertigo, accounting for approximately 20-30% of all dizziness cases [1]. This condition occurs when tiny calcium carbonate crystals (called otoconia or “ear rocks”) become dislodged from their normal location in the utricle and migrate into one of the semicircular canals.
Symptoms of BPPV:
- Brief episodes of intense spinning sensation (lasting less than one minute)
- Triggered by specific head movements (rolling over in bed, looking up, bending down)
- Nausea and sometimes vomiting
- Abnormal eye movements (nystagmus) during episodes
- Symptoms that come and go over weeks or months
What Causes BPPV?
- Age-related degeneration (most common in people over 50)
- Head injury or trauma
- Inner ear infection or inflammation
- Prolonged bed rest
- Sometimes no identifiable cause (idiopathic)
The good news? BPPV is highly treatable with specific head maneuvers performed by a healthcare provider, with success rates exceeding 80% [2].
Meniere’s Disease
Meniere’s disease is a chronic inner ear disorder characterized by abnormal fluid buildup (endolymphatic hydrops) in the inner ear. This condition typically affects only one ear initially, though it can eventually involve both ears in about 30% of cases [3].
Classic Symptoms of Meniere’s Disease:
- Episodic vertigo lasting 20 minutes to several hours
- Fluctuating hearing loss, particularly in low frequencies
- Tinnitus (ringing, roaring, or buzzing in the ear)
- Aural fullness (feeling of pressure or fullness in the ear)
These four symptoms together are sometimes called the “Meniere’s tetrad.” If you’re experiencing ear ringing, it could be related to this condition.
Meniere’s Disease Progression:
| Stage | Characteristics | Duration |
|---|---|---|
| Early | Sudden attacks of vertigo, temporary hearing loss that recovers | Months to years |
| Middle | Vertigo attacks continue, hearing loss becomes more permanent | Years |
| Late | Vertigo episodes may decrease, but balance problems persist, significant permanent hearing loss | Ongoing |
Vestibular Neuritis and Labyrinthitis
These two conditions are often confused because they share similar symptoms, but there’s an important difference:
Vestibular Neuritis affects only the vestibular nerve (balance), while Labyrinthitis affects both the vestibular nerve and the cochlear nerve (hearing).
Symptoms:
- Sudden, severe vertigo that can last days
- Significant balance problems
- Nausea and vomiting
- Difficulty walking or standing
- Hearing loss and tinnitus (in labyrinthitis only)
Both conditions are typically caused by viral infections that inflame the inner ear nerves. The inflammation disrupts normal signal transmission to the brain, causing intense dizziness. Understanding symptoms of ear nerve damage can help you recognize these conditions early.
Superior Semicircular Canal Dehiscence (SSCD)
This rare condition occurs when there’s an abnormal opening in the bone covering the superior semicircular canal. This opening creates a “third window” in the inner ear, disrupting normal fluid movement and pressure.
Unique Symptoms of SSCD:
- Vertigo triggered by loud sounds (Tullio phenomenon)
- Dizziness from pressure changes (coughing, sneezing, straining)
- Hearing your own voice or bodily sounds too loudly (autophony)
- Pulsatile tinnitus (hearing your heartbeat)
- Balance problems
Perilymph Fistula
A perilymph fistula is an abnormal connection between the fluid-filled inner ear and the air-filled middle ear, usually occurring at the oval or round window. This allows perilymph fluid to leak into the middle ear.
Causes:
- Head trauma or injury
- Barotrauma (pressure changes from diving, flying)
- Chronic ear infections
- Strenuous physical activity
- Sometimes congenital (present from birth)
Symptoms:
- Vertigo triggered by coughing, sneezing, or straining
- Fluctuating hearing loss
- Imbalance and unsteadiness
- Fullness or pressure in the ear
How Ear Disorders That Cause Dizziness Are Diagnosed 🔍
Accurate diagnosis is essential for effective treatment. Healthcare providers use a combination of clinical examination, specialized tests, and sometimes imaging to identify the specific ear disorder causing your dizziness.
Medical History and Physical Examination
Your doctor will start with detailed questions about:
- Symptom characteristics: What does your dizziness feel like? Spinning (vertigo) or lightheadedness?
- Timing and duration: How long do episodes last? What triggers them?
- Associated symptoms: Hearing loss, tinnitus, ear fullness, headaches?
- Medical history: Recent infections, head injuries, medications?
The physical examination includes:
- Dix-Hallpike maneuver: Tests for BPPV by moving your head into positions that might trigger vertigo
- Head impulse test: Assesses vestibular nerve function
- Romberg test: Evaluates balance with eyes open and closed
- Gait assessment: Observes how you walk and maintain balance
Specialized Vestibular Testing
Videonystagmography (VNG) or Electronystagmography (ENG): These tests record eye movements while you follow visual targets, change head positions, or receive warm and cool air in your ears. Abnormal eye movements help identify which part of the vestibular system is affected.
Vestibular Evoked Myogenic Potentials (VEMP): Measures muscle responses to sound or vibration, helping diagnose conditions like SSCD or Meniere’s disease.
Rotary Chair Testing: You sit in a motorized chair that rotates at controlled speeds while your eye movements are recorded, providing detailed information about vestibular function.
Posturography: Assesses how well you maintain balance under different sensory conditions using a specialized platform.
Hearing Tests
Since many ear disorders that cause dizziness also affect hearing, audiological testing is crucial:
- Pure-tone audiometry: Determines hearing thresholds at different frequencies
- Speech audiometry: Assesses ability to understand speech
- Tympanometry: Evaluates middle ear function
- Otoacoustic emissions: Tests inner ear (cochlear) function
If you’re experiencing hearing loss in one ear, this could provide important diagnostic clues.
Imaging Studies
MRI (Magnetic Resonance Imaging): Can detect tumors (like acoustic neuromas), inflammation, or structural abnormalities affecting the inner ear or vestibular nerve.
CT Scan: Particularly useful for identifying bone abnormalities like SSCD or temporal bone fractures.
High-resolution imaging: Specialized MRI techniques can visualize endolymphatic hydrops in Meniere’s disease.
Treatment Options for Ear Disorders That Cause Dizziness 💊
Treatment varies significantly depending on the specific diagnosis, but the goal is always to reduce symptoms, improve balance, and enhance quality of life.
Treatments for BPPV
Canalith Repositioning Procedures: These are the gold standard for BPPV treatment.
- Epley maneuver: A series of head movements that guide displaced crystals back to their proper location
- Semont maneuver: An alternative repositioning technique
- Brandt-Daroff exercises: Home exercises that can help prevent recurrence
Success rates for these maneuvers range from 80-90% with one to three treatments [4]. Many patients experience immediate relief.
Treatments for Meniere’s Disease
Meniere’s disease requires a multi-faceted approach:
Dietary Modifications:
- Low-sodium diet (less than 2,000 mg per day)
- Limiting caffeine and alcohol
- Staying well-hydrated
- Avoiding trigger foods
Medications:
- Diuretics: Help reduce fluid retention
- Anti-vertigo medications: Meclizine or diazepam for acute attacks
- Anti-nausea medications: Promethazine or ondansetron
Advanced Treatments:
- Intratympanic gentamicin: Injections into the middle ear to reduce vestibular function
- Intratympanic corticosteroids: Anti-inflammatory injections
- Endolymphatic sac surgery: Decompression procedure
- Vestibular nerve section: Surgical option for severe, uncontrolled cases
Treatments for Vestibular Neuritis and Labyrinthitis
Acute Phase (first few days):
- Corticosteroids: Reduce inflammation (most effective when started early)
- Antivirals: May be prescribed if viral infection is suspected
- Vestibular suppressants: Short-term use of meclizine or diazepam
- Anti-nausea medications: For symptom relief
Recovery Phase:
- Vestibular rehabilitation therapy (VRT): Specialized physical therapy exercises that help your brain compensate for inner ear damage
- Gradual return to activities: As symptoms improve
- Balance exercises: To prevent falls and improve stability
Vestibular Rehabilitation Therapy (VRT) 🏋️
VRT is a specialized form of physical therapy effective for many ear disorders that cause dizziness. It works by promoting central nervous system compensation for inner ear deficits.
VRT exercises include:
- Gaze stabilization: Focusing on a target while moving your head
- Balance training: Standing on different surfaces with varying visual input
- Habituation exercises: Repeatedly performing movements that trigger mild dizziness
- General conditioning: Improving overall fitness and endurance
Studies show VRT significantly improves symptoms in 60-90% of patients with chronic vestibular disorders [5].
Medications for Dizziness Management
| Medication Class | Examples | Primary Use | Duration |
|---|---|---|---|
| Antihistamines | Meclizine, dimenhydrinate | Acute vertigo episodes | Short-term only |
| Benzodiazepines | Diazepam, lorazepam | Severe acute vertigo | Very short-term |
| Antiemetics | Promethazine, ondansetron | Nausea and vomiting | As needed |
| Diuretics | Hydrochlorothiazide | Meniere’s disease | Long-term |
| Corticosteroids | Prednisone, methylprednisolone | Inflammation | Short courses |
Important note: Vestibular suppressants should only be used short-term (3-5 days) because prolonged use can delay central compensation and prolong recovery.
Surgical Options
Surgery is reserved for severe cases that don’t respond to conservative treatments:
- Labyrinthectomy: Removes the balance portion of the inner ear (for severe Meniere’s with poor hearing)
- Vestibular nerve section: Cuts the vestibular nerve while preserving hearing
- SSCD repair: Closes the abnormal opening in the bone
- Perilymph fistula repair: Seals the leak between inner and middle ear
Living with Ear Disorders That Cause Dizziness: Practical Strategies 🏠
Beyond medical treatments, lifestyle modifications and coping strategies can significantly improve daily functioning.
Safety Modifications at Home
- Remove trip hazards: Secure loose rugs, clear clutter from walkways
- Install grab bars: In bathrooms and along stairways
- Improve lighting: Use night lights and ensure adequate illumination
- Non-slip surfaces: Bath mats, non-skid shoes
- Avoid ladders: When possible, or use extra caution
Dietary and Lifestyle Considerations
Foods and substances to limit (especially for Meniere’s disease):
- Sodium (salt)
- Caffeine
- Alcohol
- MSG and other additives
- Nicotine
Beneficial habits:
- Stay well-hydrated
- Maintain regular sleep schedule
- Manage stress through relaxation techniques
- Regular, moderate exercise (as tolerated)
- Consider hearing support supplements after consulting your doctor
Managing Acute Vertigo Episodes
When a vertigo attack strikes:
- Stop what you’re doing and sit or lie down immediately
- Keep your head still and focus on a stationary object
- Avoid bright lights and loud noises
- Stay in a safe position until the episode passes
- Don’t drive or operate machinery during or immediately after an episode
- Take prescribed medications as directed
Emotional and Psychological Support
Living with chronic dizziness can be emotionally challenging. Many people experience:
- Anxiety about when the next episode will occur
- Depression from activity limitations
- Social isolation due to fear of symptoms in public
- Frustration with diagnosis delays or treatment failures
Helpful strategies:
- Join support groups (online or in-person)
- Consider counseling or cognitive behavioral therapy
- Educate family and friends about your condition
- Set realistic expectations and celebrate small improvements
- Practice stress-reduction techniques like meditation or yoga
When to Seek Medical Attention ⚠️
While occasional mild dizziness may not be concerning, certain symptoms warrant immediate medical evaluation:
Seek emergency care if you experience:
- Sudden, severe vertigo with headache, confusion, or difficulty speaking
- Vertigo accompanied by chest pain or shortness of breath
- Dizziness with sudden hearing loss in one ear
- Loss of consciousness
- Severe vomiting that prevents keeping fluids down
- Symptoms following head trauma
- Weakness, numbness, or vision changes
Schedule an appointment with your doctor if:
- Dizziness persists for more than a few days
- Episodes are becoming more frequent or severe
- You’re experiencing hearing changes or tinnitus
- Balance problems are affecting daily activities
- You’ve had multiple falls
- Symptoms aren’t improving with treatment
Understanding the causes of hearing loss in one ear can help you recognize when ear-related dizziness requires professional evaluation.
The Connection Between Hearing Loss and Dizziness
Many ear disorders that cause dizziness also affect hearing because the structures responsible for both functions are located in the same area—the inner ear. Understanding this connection is crucial for comprehensive treatment.
Shared Anatomy and Physiology
The cochlea (responsible for hearing) and the vestibular system (responsible for balance) are connected within the bony labyrinth of the inner ear. They share:
- The same blood supply
- Similar fluid systems (endolymph and perilymph)
- Connected nerve pathways (both branch from the vestibulocochlear nerve)
- Susceptibility to the same diseases and conditions
This is why conditions like labyrinthitis, Meniere’s disease, and acoustic neuroma affect both hearing and balance simultaneously.
Recognizing Combined Symptoms
If you’re experiencing both dizziness and hearing changes, pay attention to:
- Timing: Do they occur together or separately?
- Affected ear: Is it the same ear or different ears?
- Pattern: Are symptoms constant or episodic?
- Progression: Are they getting worse, staying stable, or improving?
This information helps your healthcare provider make an accurate diagnosis. The most common cause of hearing loss may differ from the most common cause of dizziness, but when they occur together, it narrows the diagnostic possibilities.
Impact on Treatment Approach
When both hearing and balance are affected, treatment must address both issues:
- Hearing aids: May be recommended even while treating vestibular symptoms
- Cochlear implants: For severe hearing loss, with consideration of balance function
- Coordinated care: Between audiologists, ENT specialists, and vestibular therapists
- Monitoring: Regular hearing tests to track changes
Prevention and Long-Term Management Strategies
While not all ear disorders that cause dizziness can be prevented, certain strategies can reduce risk and improve long-term outcomes.
Protecting Your Ears
Avoid excessive noise exposure:
- Use hearing protection in loud environments
- Keep headphone volume at safe levels (no more than 60% of maximum)
- Take breaks from noisy activities
- Understand hearing damage prevention
Prevent ear infections:
- Treat respiratory infections promptly
- Keep ears dry after swimming
- Don’t insert objects into ear canals
- Manage allergies effectively
Protect against head injuries:
- Wear helmets during sports and cycling
- Use seatbelts in vehicles
- Fall-proof your home
- Practice workplace safety
Managing Underlying Health Conditions
Several systemic conditions can contribute to ear disorders and dizziness:
- Cardiovascular disease: Maintain healthy blood pressure and cholesterol
- Diabetes: Keep blood sugar well-controlled
- Autoimmune disorders: Follow treatment plans carefully
- Migraines: Identify and avoid triggers (vestibular migraine can cause dizziness)
Regular Health Monitoring
Schedule regular check-ups:
- Annual hearing tests, especially if you’re over 50
- Blood pressure monitoring
- Medication reviews (some drugs affect balance)
- Vision checks (poor vision can worsen balance problems)
Staying Active Safely
Physical activity is important for overall health and balance maintenance:
- Choose appropriate exercises: Swimming, walking, tai chi, yoga
- Start slowly: Gradually increase intensity and duration
- Use support: Handrails, walking poles, or a buddy system
- Listen to your body: Stop if you feel dizzy or unsteady
For seniors, effective hearing health strategies include maintaining both hearing and balance function.
Emerging Research and Future Treatments
The field of vestibular medicine continues to evolve, with promising research into new diagnostic tools and treatments for ear disorders that cause dizziness.
Advances in Diagnostic Technology
- Virtual reality testing: More precise assessment of vestibular function
- Smartphone-based apps: Home monitoring of symptoms and balance
- Genetic testing: Identifying hereditary forms of vestibular disorders
- Advanced imaging: Better visualization of inner ear structures
Novel Treatment Approaches
Regenerative medicine:
- Stem cell therapy to repair damaged inner ear structures
- Gene therapy for hereditary vestibular conditions
- Growth factors to promote nerve regeneration
Improved medications:
- Targeted drugs with fewer side effects
- Medications that promote vestibular compensation
- Better treatments for Meniere’s disease
Enhanced rehabilitation:
- Virtual reality-based vestibular therapy
- AI-powered personalized exercise programs
- Wearable devices that provide real-time balance feedback
Clinical Trials and Research Participation
If you’re interested in contributing to vestibular research, consider:
- Asking your doctor about relevant clinical trials
- Registering with research databases
- Participating in patient registries
- Supporting vestibular research organizations
Understanding the Prognosis: What to Expect
The outlook for people with ear disorders that cause dizziness varies significantly depending on the specific condition, severity, and individual factors.
BPPV Prognosis
- Excellent short-term outlook: 80-90% resolution with treatment
- Recurrence common: About 50% experience recurrence within 5 years
- Easily retreatable: Repeated maneuvers are effective
- No permanent damage: BPPV doesn’t cause lasting hearing or balance problems
Meniere’s Disease Prognosis
- Variable course: Symptoms fluctuate over time
- Hearing loss: Often progressive in affected ear(s)
- Vertigo improvement: Episodes often decrease in frequency over years
- Balance issues: May persist even when vertigo improves
- Quality of life: Can be significantly impacted but improves with treatment
Vestibular Neuritis/Labyrinthitis Prognosis
- Acute phase: Severe symptoms typically last 3-7 days
- Recovery: Gradual improvement over weeks to months
- Compensation: Brain usually adapts well with rehabilitation
- Residual symptoms: Some people have mild, persistent imbalance
- Hearing recovery: Variable in labyrinthitis; some permanent loss is possible
Factors Affecting Recovery
Positive prognostic factors:
- Early diagnosis and treatment
- Younger age
- Good overall health
- Active participation in rehabilitation
- Strong social support
Challenging factors:
- Delayed treatment
- Multiple vestibular problems
- Other neurological conditions
- Advanced age
- Limited mobility or activity
Complementary and Alternative Approaches

While conventional medical treatment should always be the foundation, some people find additional relief from complementary therapies. Always discuss these with your healthcare provider before trying them.
Potentially Helpful Approaches
Acupuncture: Some studies suggest it may help reduce vertigo symptoms in certain conditions [6].
Ginkgo biloba: Limited evidence for vertigo reduction, but may help some people. Consult your doctor about interactions with other medications.
Vitamin D supplementation: Research suggests vitamin D deficiency may be associated with BPPV recurrence [7]. Supplementation might help prevent recurrences.
Stress reduction techniques:
- Meditation and mindfulness
- Progressive muscle relaxation
- Biofeedback
- Breathing exercises
Dietary supplements: Some people explore natural remedies for tinnitus and related symptoms, though scientific evidence varies.
Approaches to Use with Caution
- Chiropractic neck manipulation (may worsen some conditions or even cause stroke)
- Unproven herbal remedies without medical supervision
- Extreme dietary restrictions without professional guidance
- Delaying conventional treatment in favor of alternative approaches
Building Your Healthcare Team
Managing ear disorders that cause dizziness often requires coordinated care from multiple specialists.
Key Healthcare Providers
Primary Care Physician: Your first point of contact, coordinates overall care, manages general health conditions.
Otolaryngologist (ENT): Ear, nose, and throat specialist who diagnoses and treats ear disorders.
Neurotologist: ENT subspecialist focusing specifically on ear and balance disorders.
Audiologist: Performs hearing and balance testing, fits hearing aids.
Vestibular Physical Therapist: Provides specialized rehabilitation exercises.
Neurologist: Evaluates for neurological causes of dizziness.
Psychologist/Counselor: Addresses emotional and psychological impacts.
Maximizing Your Medical Appointments
Before your appointment:
- Keep a symptom diary (when, what, how long, triggers)
- List all medications and supplements
- Write down questions
- Bring a family member or friend for support
During your appointment:
- Describe symptoms clearly and specifically
- Be honest about symptom severity and impact
- Ask about treatment options and their pros/cons
- Request written instructions or educational materials
- Clarify follow-up plans
After your appointment:
- Follow treatment plans as prescribed
- Report new or worsening symptoms promptly
- Keep scheduled follow-up appointments
- Track your progress
The Psychological Impact of Chronic Dizziness
Living with ear disorders that cause dizziness extends beyond physical symptoms—it significantly affects mental health and quality of life.
Common Psychological Effects
Anxiety and panic: Fear of when the next episode will strike, especially in public places or while driving.
Depression: Frustration with limitations, loss of independence, and chronic symptoms.
Social isolation: Avoiding activities, events, or places due to fear of symptoms.
Reduced self-confidence: Uncertainty about physical abilities and safety.
Relationship strain: Impact on family dynamics, work relationships, and social connections.
Coping Strategies
- Education: Understanding your condition reduces fear and uncertainty
- Realistic expectations: Accept that recovery may take time
- Pacing: Balance activity with rest; don’t overdo it
- Communication: Help others understand your limitations and needs
- Maintain connections: Stay socially engaged within your capabilities
- Professional support: Don’t hesitate to seek counseling or therapy
- Support groups: Connect with others facing similar challenges
For comprehensive information and support, visit Improve Hearing Health for additional resources.
Frequently Asked Questions About Ear Disorders That Cause Dizziness
Q: Can ear disorders that cause dizziness be cured?
A: It depends on the specific condition. BPPV can often be “cured” with repositioning maneuvers, though it may recur. Conditions like Meniere’s disease are chronic but manageable. Vestibular neuritis often resolves with time and rehabilitation. Complete recovery varies by individual and condition.
Q: How long does dizziness from ear problems last?
A: Duration varies widely: BPPV episodes last seconds to minutes; Meniere’s attacks last 20 minutes to hours; vestibular neuritis causes severe symptoms for days with gradual recovery over weeks to months. Chronic conditions may cause persistent mild symptoms.
Q: Can stress cause ear-related dizziness?
A: While stress doesn’t directly cause most ear disorders, it can trigger or worsen symptoms in conditions like Meniere’s disease and vestibular migraine. Stress also affects how you perceive and cope with dizziness.
Q: Is dizziness from ear problems dangerous?
A: The dizziness itself usually isn’t dangerous, but it increases fall risk and can make certain activities (like driving) unsafe. Some underlying causes (like tumors) require treatment. Always get persistent or severe dizziness evaluated.
Q: Can ear infections cause permanent dizziness?
A: Most ear infections resolve without permanent effects. However, severe or untreated infections can damage inner ear structures, potentially causing lasting balance problems or hearing loss. Early treatment is important.
Q: Will I need surgery for my ear-related dizziness?
A: Most people don’t need surgery. Conservative treatments (medications, dietary changes, repositioning maneuvers, vestibular therapy) are effective for the majority of patients. Surgery is reserved for severe cases that don’t respond to other treatments.
🏥 Ear Disorder Symptom Checker
Answer these questions to identify which ear disorder might be causing your dizziness
Your Possible Conditions:
Conclusion: Taking Control of Your Balance Health
Ear disorders that cause dizziness can be frightening, disruptive, and frustrating, but understanding these conditions is the first step toward effective management and recovery. Whether you’re experiencing brief spinning episodes from BPPV, the episodic vertigo of Meniere’s disease, or the prolonged dizziness of vestibular neuritis, remember that you’re not alone and help is available.
Key Action Steps Moving Forward
1. Seek Professional Evaluation: Don’t dismiss persistent or severe dizziness. Early diagnosis leads to better outcomes and can prevent complications.
2. Be Your Own Advocate: Keep detailed symptom records, ask questions, and actively participate in your treatment plan. Your observations are valuable diagnostic clues.
3. Commit to Treatment: Whether it’s repositioning maneuvers, medications, dietary changes, or vestibular rehabilitation, consistency with your treatment plan is crucial for success.
4. Make Safety a Priority: Modify your environment to prevent falls, avoid driving during symptomatic periods, and use assistive devices when needed.
5. Address the Whole Person: Don’t neglect the emotional and psychological aspects of living with chronic dizziness. Seek support when needed and maintain social connections.
6. Stay Informed: Medical understanding of vestibular disorders continues to evolve. Stay connected with your healthcare team and reputable sources like Improve Hearing Health for updated information.
7. Practice Patience: Recovery from ear disorders that cause dizziness often takes time. Your brain needs weeks or months to compensate for inner ear changes. Trust the process and celebrate small improvements.
Looking Ahead with Hope
While living with ear-related dizziness presents challenges, the majority of people find significant relief through appropriate treatment. Advances in diagnostic techniques, new therapeutic approaches, and better understanding of vestibular disorders mean that the outlook continues to improve.
Remember that your balance system is remarkably adaptable. With proper treatment, rehabilitation, and time, your brain can learn to compensate for inner ear problems, allowing you to return to the activities you enjoy. Whether you’re dealing with a temporary condition like BPPV or managing a chronic disorder like Meniere’s disease, effective strategies exist to help you regain stability and confidence.
Take that first step today—reach out to a healthcare provider, start keeping a symptom diary, or explore the resources available to you. Your journey to better balance begins with understanding, continues with action, and leads to improved quality of life. You have the power to take control of your vestibular health and move forward with confidence, one steady step at a time.
For more information about understanding tinnitus and seeking relief, visit our comprehensive resource center.
References
[1] Bhattacharyya, N., et al. (2017). “Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update).” Otolaryngology–Head and Neck Surgery, 156(3_suppl), S1-S47.
[2] Hilton, M. P., & Pinder, D. K. (2014). “The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo.” Cochrane Database of Systematic Reviews, (12).
[3] Nakashima, T., et al. (2016). “Meniere’s disease.” Nature Reviews Disease Primers, 2(1), 1-18.
[4] von Brevern, M., et al. (2015). “Short-term efficacy of Epley’s manoeuvre: a double-blind randomised trial.” Journal of Neurology, Neurosurgery & Psychiatry, 76(10), 1365-1370.
[5] McDonnell, M. N., & Hillier, S. L. (2015). “Vestibular rehabilitation for unilateral peripheral vestibular dysfunction.” Cochrane Database of Systematic Reviews, (1).
[6] Xu, Y., et al. (2016). “Acupuncture for peripheral vertigo: A systematic review and meta-analysis.” Evidence-Based Complementary and Alternative Medicine, 2016.
[7] Jeong, S. H., et al. (2013). “Decreased serum vitamin D in idiopathic benign paroxysmal positional vertigo.” Journal of Neurology, 260(3), 832-838.